Maintenance
Declination
Percent
of
Function
100
75
50
25
75
50
25
Post Injury (Years)
Model of Aging and Physical Disability
ARTICLE #5: Aging with Spinal Cord Injury
Table of Contents
Section #1: Issues of Aging with Spinal Cord Injury
Robert R. Menter
“It was the best of times, it was the worst of times, it was the age of wisdom, it was the age of foolishness . . . .”
So it was that Charles Dickens used contrast to open Tale of Two Cities and so it is that we open the story of aging with spinal cord injury. From the optimism of youth to the wisdom of age, from the excitement of new challenges to the security of the routine, from the focus on cure to an emphasis on care – through the years, the tempo changes.
Aging represents many faces and moods. To understand aging requires an understanding of the childhood story of the blind man and the elephant. Six blind men examined an elephant with their hands. One described its likeness to a wall, one to a snake, and the others to a spear, a tree, a fan, and a rope. So it is that we hear many different accounts of the impact of aging in spinal cord injury. For one, it is deterioration of shoulders interfering with transfers and independence. For another, it is the loss of skin tolerance, limiting sitting time; for another, it is the loss of a parent who has provided loving care and emotional support; for another, it is the inability to live independently because of dwindling financial resources.
While we often focus on the negatives of aging, there are positives such as wisdom, maturity, and the satisfaction of survival. That mixture of positive and negative gives new meaning to the term bittersweet. To lay a groundwork for understanding these changes, this chapter will try to provide a framework with which to view the changes.
DEMOGRAPHICS
The Spinal cord injury (SCI) population of the United States has been estimated at 173,000 individuals, based on a prevalence of 721 SCIs per million and a 1990 United States Census population of 240 million. To this, approximately 10,000 cases are added per year with an estimated economic impact of spinal cord injury of $4 billion per year (1).
In 1999 the Paralysis Society of America (PSA) of the Paralyzed Veterans of America (PVA) completed a study titled “The Economic Consequences of Traumatic Spinal Cord Injury” (2). The study established the prevalence cited above and established a multiple data profile, which helps us understand the evolving distribution and age of people with SCI. Two profiles of particular interest are displayed in Table 1.1 and Table 1.2.
Table 1.1 reveals that 1 out of 4 SCI survivors is over 20 years post-injury. Twenty years post-injury appears to be a point at which some of the aging problems begin to increase; thus, a significant portion of SCI survivors are rapidly approaching the problems of aging.
Table 1.2 shows that the distribution of SCI is not exclusively young people. Even when injuries occur at youthful ages, young men and women with SCI continue to grow older, emphasizing the need for service delivery to people of all ages. Indeed, some 40% of all SCI survivors are over 45 years of age.
Table 1.1. SCI Population: Year of Injury |
|
Year of Injury |
Percent |
Before 1970 |
24.3 |
| After 1970 | 75.7 |
A second issue to be examined in the overall topic of aging and SCI is that of older onset injuries. Because of the so-called “graying” of America, the general population is growing older; an estimated 30 million people currently are over the age of 65 (3). Age-related physiologic changes include increased cervical arthritis, which decreases the size of the spinal canal, and impaired mobility and balance, both of which cause falls. These physiologic changes act together to increase the number of spinal cord injuries. Moreover, older individuals have a much greater risk of paralysis from relatively minimal traumas than do younger people. Review of data from the National Spinal Cord Injury Database in Birmingham, Alabama, confirms the increased number of SCI onset at older ages (Table 1.3) (4,5).
Initial impressions indicate that individuals with SCI onset in later years have very different patterns of outcome, programmatic needs, and resources than do those with onset in their younger years. In order to understand the current interplay of SCI and aging, it is important to have a historical perspective of the issues as they have evolved.
HISTORY OF SPINAL CORD INJURY
The 1940s heralded the onset of modern SCI care, led by Sir Ludwig Guttman at Stoke Mandeville in England, in the United States by Dr. Ernest Bors in the VA Hospital in Birmingham, California, and by Dr. Donald Munro at the Boston University Medical Center.
The medical model of care and service delivery has been the dominant theme from the inception of SCI care to the present day. Because the original focus of care and survival was in the military hospital, it was only natural that decision-making and organizational management follow military medical tradition. Even when significant numbers of nonmilitary SCI survivors began to appear, the model of decision-making and organizational management still closely followed the military model: paternalism was the key ethical concept, with the physician making the decisions and performing the role of gatekeeper.
| Table 1.2. SCI Population: Current Age | |
Current
Age (1988) |
% |
0-15 |
0.1 |
16-30 |
19.8 |
31-45 |
40.0 |
46-60 |
19.7 |
61+ |
20.4 |
Each decade from the 1940s through the 1980s has been accompanied by major changes in the medical treatment resources available to deal with spinal cord injury and paralysis. As a result of the changing resources, each decade has seen the emergence of different survival profiles. Equally important, the goals and outcomes have been revised each decade to reflect changing expectations.
Medical resources in the 1940s were limited in that sulfa was the principle medication available to combat infection. Although penicillin was available during the latter portion of the war, it was not widely available for civilian use until the late 1940s. Survivors in the 1940s, for the most part, were persons with mid- and lower-level paraplegia, and the primary functional rehabilitation goal was survival within institutional settings. By the very nature of the rehabilitation goals, the individuals were very sedentary.
The 1950s witnessed the introduction of streptomycin and tetracycline to boost the already widely available penicillin in the treatment of infections. With limited antibiotics, the spinal-cord-injured population expanded to include the persons with high-level paraplegia and the rehabilitation goals changed from institutionalization to survival in the individual's home. However, in the home, the individual with SCI remained dependent upon family members for care. Activities remained sedentary and the term “medically necessary” was developed to describe those resources needed to get the individual from the institution to the home environment.
The 1960s were marked by the development of a full complement of antibiotics and survival of persons with low-level quadriplegia in significant numbers. Rehabilitation goals began to expand beyond the home to include involvement in the community. Although person with paraplegia who were independent in self-care began to live outside the home, those individuals with quadriplegia continued to live at home, depending on members of their family for care.
| Table 1.3. National SC Database: Age at Injury |
||
Age |
1981 (N = 6012) |
1991 (N = 13,761) |
0-15 |
5.9 |
4.6 |
16-30 |
62.4 |
59.3 |
31-45 |
18.3 |
20.5 |
46-60 |
9.0 |
9.6 |
61-75 |
3.7 |
4.7 |
76-98 |
0.7 |
1.3 |
The 1970s were noted by the development of modern Emergency Medical Services (EMS) with respiratory support programs. EMS provided prompt response to the scene of an accident by individuals trained in extraction and life support measures. Accordingly, increasing numbers of persons with middle and high level quadriplegia survived. They, too, returned to the community. During the 1970s, the rehabilitation goals evolved to include the concepts of “super para” and “super quad,” whereby individuals were encouraged to exceed expected functional goals for their level of injury.
Examples of super paras were individuals injured at the T10 level spending nearly all of their time up and about in long leg braces and crutches. Super quads might be represented by persons with complete C6 quadriplegia living alone with no attendant care. In both situations, the high levels of function required tremendous energy expenditure, and there was little or no margin of safety. Anything that impaired optimal function such as weight gain or increased spasms created a potential setback or injury.
The 1970s also introduced independent living programs and support services outside the home. Previously, such services outside the home and family were essentially nonexistent. With increased independence and development of attendant care in the community, people moved out of their homes and became less dependent upon family structures for care. The early concepts of quality of life began to evolve and, with them, recognition that quality of life requires additional support beyond the medical model of care and the term “medically necessary.”
The 1980s saw a significant change in the type of initial neurologic injury. Where neurologically complete spinal cord injuries had predominated, incomplete spinal cord injuries began to increase in number. Many more individuals had sensation and/or movement present or experienced later recovery of these functions distal to the spinal injury site. Data from the National SCI Database, presented in Table 1.4, reflect the changing proportions of complete and incomplete injuries between 1973 and 1988 (6.)
Also occurring in the 1980s was the first recognition of aging as a problem. With some awareness of aging has come the real concern that super para and super quad lifestyles may produce wear and tear that accelerates the aging problem.
In studying problems associated with aging in SCI, the survivors of the 1950s are primarily persons with paraplegia and are now approaching 30-40 years post-injury; whereas, older surviving people with mid-level quadriplegia are approximately 20 years post-injury, and the oldest surviving individuals with high quadriplegia are 10 years post-injury.
To perform aging research in SCI, it must be recognized that the goals and outcomes of each decade create their own patter of complications. An example would be the persons with paraplegia of the 1940s who were sent home to “survive” and were very sedentary. They will have different patterns of wear and tear than the super paras of the 1970s, who pushed themselves beyond ordinary levels of function to overachieve.
Early awareness of the potential problems of aging and spinal cord injury was focused by George Hohmann, Ph.D. in 1982 (7). He recounted the experiences of fellow World War II SCI survivors, outlining orthopedic problems, neurologic complications, medical infections, obesity, family issues, and psychosocial problems all adversely affecting the lifestyles and well-being of these individuals. Closely following Dr. Hohmann were Roberta Trieschmann, Ph.D., author of Aging with a Disability, and Barry Corbet, filmmaker and author of Options Revisited [Survivors], who further explored the interface of aging and SCI (8-10). Others have followed, ultimately leading to this multiauthored book attempting to define the state of knowledge in 1992 (11-14).
| Table 1.4. National SCI Database: Admission Neurologic Function Below Level of Injury | ||
Year |
% Complete |
% Incomplete |
1973 |
62 |
68 |
1980 |
50 |
50 |
1988 |
44 |
56 |
The Aging Process
Aging involves at least three major life-long developmental processes, all overlapping, but all distinctly different:
Physiologic changes are the most commonly discussed manifestation of aging. Examples of such physiologic change are loss of muscle mass with resultant decrease in strength, decreased range of motion and osteoarthritis leading to pain and decreased function, and increased urologic and bowel problems. All of these are biophysical changes in the body and, as such, are measurable. The spectrum of physiologic changes which occurs with age in the nondisabled population is described in the following chapters. Unfortunately it is largely unknown what these “normal” physiologic changes will do when superimposed upon an individual with SCI. Are they additive and do they accelerate deterioration of a particular organ system?
Changing social roles are as inevitable as physiologic changes as one moves from childhood to young adulthood, to adult, and to elderly roles in the family and community. Sociologic events include leaving home, marrying, parenting, losing one's parents, and/or losing a spouse. Each sociologic change may have significant implications in the aging process.
Self-realization is a topic rarely discussed, but is perhaps the most important of the aging factors. It includes the issues of developing values, ethics, morality, and ultimately finding meaning in life. This is the growing up of the mind. It is also referred to as spiritual growth and has the potential of making physiologic and sociologic changes less devastating.
Perhaps the most distinct feature of aging is the increased uniqueness and differentiation of each individual within the aging patter and process. Looking at 100 20-year-old persons with C6 quadriplegia, there would be 100 persons with a very similar profile of functional abilities, health impairment, and organ system reserves. To look at the same group 30 years later, one would see tremendous variation in the diseases of individuals, such as hypertension, obesity, heart disease, bowel dysfunction, and urologic disease, as well as tremendous variations in functional abilities. Because of this diversity and differentiation, it may be very difficult to predict aging changes in any individual.
Major components determining the aging process include:
• Genetic factors
• Lifestyle
• Adaption to stress
• Sociologic role
• Trauma
Recognizable genetic characteristics of aging within families include
Many times other characteristics of parents or families may be perpetuated, such as smoking, drinking, eating excessively, or not responding to stress well; however, those characteristics are not genetic, but are acquired.
Lifestyle refers to how closely life's activities are balanced against each other: are physical, psychological, and social needs balanced, or are risks taken such as smoking, drinking, eating adversely, and living dangerously? Risk-taking has the potential of adversely affecting the well-being of an individual and speeding up the aging process.
Stress in the aging process is particularly important. Unmanaged stress may lead to such diverse medical problems as hypertension, heart disease, obesity, peptic ulcer disease, and respiratory disease. Each of these medical conditions can significantly influence and interfere with an individual's quality of life. Unmanaged stress may also create destructive lifestyles and increase the risk of trauma.
Sociologic role relates to relationships formed and how they affect our lives. An example would be the observation that stable, healthy marriages create much less aging or deterioration than stressful, unhealthy marriages. Relationships frequently reinforce choices of lifestyle, stress management, and risks of trauma.
Although trauma typically refers to physical injury to the body, it also should include emotional trauma. SCI induces both physical and emotional trauma and instant loss of multiple system reserves, giving the equivalent of multiple years of aging. Examples of trauma after SCI would include repeated skin breakdown and decubiti leading to scarring and immobility of the skin, or repeated injury to the shoulders from transfers or other activities that tear muscles permanently, and thus interfere with shoulder function.
PHYSIOLOGIC CHANGES
Research has identified the typical aging patterns in all systems of the body. In any given individual, however, the particular pattern of aging will vary. For example, in an individual with severe asthma, the pulmonary systems will be exhausted at an early age, which then impacts the overall body function; or, in an individual with rheumatoid arthritis, the patter of aging may be expressed by decreased range of motion and increased pain, both of which lead to decreased overall function. With SCI, there may be dramatic changes in many systems such as skin sensitivity, bladder function, bowel function and loss of extremity movement – all acting to interfere with the overall mobility and health of the individual. Nonetheless, because there is a tremendous amount of reserve built into each organ system, and because of the complex system of adaptation offered by rehabilitation, most individuals continue to function, even if at a reduced capacity.
CHANGING SOCIAL ROLES
The changing social roles of growing older are less understood and more varied than physiological changes. The social unit after the injury occurs continues to evolve and will vary tremendously with age at onset and level of injury. Injury at a particular stage in life creates a different set of demands, expectations, and resources. For example, SCI at the teenage stage usually provides parent support and occurs at an undifferentiated stage of vocational development, in comparison to injury as a married adult and parent, when the dominant theme is holding a family together. Equally significant is the level of injury which dictates the amount of disability and the resources needed by the individual with SCI. Individuals with SCI who are completely independent in care and transportation have opportunities to form different social units than do those who are dependent in care and transportation. In the past, the perception of males with SCI as infertile has limited expectations of social roles, but with new knowledge and technology, that misperception is being corrected.
The best recognized and described event typifying changing roles is the interaction of elderly family care givers with a younger disabled family member. Frequently, there is a history of exemplary care and medical stability while an older care giver is alive, followed by a difficult transition and possible medical instability after the elderly care giver passes away or is no longer able to provide care.
Clearly, much more work needs to be done to dispel myths and to better understand the evolving and sociologic changes and how they affect the aging process in SCI.
ISSUES OF SELF-REALIZATION
Normally, the aging process is identified by decreasing physiological function, declining social roles, and what we frequently project as an expected decrease in life satisfaction. However, perhaps surprisingly, many of the aging individuals with spinal cord injuries describe increasing individual satisfaction with life despite their decline in function and social roles (10). While information is still sketchy, it appears that some of the increased satisfaction is a result of the evolution and/or maturation of self-realization as one of the three parts of the aging process. What this is and how its development can be aided will be instrumental to assisting individuals with spinal cord injury through the aging experience.
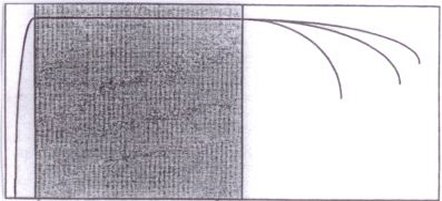
A MODEL OF AGING SCI FUNCTION
Over the years, a model of how aging may affect or impact the total function of individuals with spinal cord injuries has been developed (14). Conceptually, there are three phases following the onset of spinal injury:
Acute restoration is the process by which an individual moves from having virtually no function immediately following a spinal injury to regaining the maximum amount of function that is consistent with the level of neurologic injury. Thus, an individual with paraplegia could become independent but would still require a wheelchair or braces. An individual with C5 quadriplegia would be unable to do many things that someone with paraplegia could, but might still reach a maximum function consistent with the injury level. Usually the acute rehabilitation phase is completed within 2 years following the injury.
The maintenance phase is an indefinite but very lengthy phase. During this time, the person maintains the level of function that was established following the injury and successful rehabilitation.
The last phase, decline, occurs with the gradual onset of the physiologic aging process. With aging there are declines in muscle strength, joint range of motion, respiratory reserve, cardiovascular capacity, and skin resilience. All, either individually or collectively, cause a steady erosion of organ reserve and an overall decrease in function. Very little is known about this phase. There may or may not be recognizable patterns of decline. Nevertheless, it is important to develop an understanding of the process so that the individuals will have the option of taking actions to control or prevent some of the consequences of decline.
This model of SCI aging can be applied to groups of persons with other physical disabilities such as head injury and polio. Each disability – polio, SCI, and head injury – reflects the characteristic of a different phase. Working backward, post-polio survivors typify the last or declining phase of aging. In the 1980s, with most members approaching 40 years post-onset, this group began to exhibit aging-related concerns, for which they were totally unprepared. They were equally unprepared for the lifestyle alterations they were forced to make. changes such as increasing pain, weakness, and fatigue all exceeded what was expected for their age, and new behaviors were demanded. More physical aids were required, physical activity had to be limited, and survivors were forced to consider ways to preserve as much function and activity for the future as possible.
Fig 1.1. Model of Aging and Physical Disability.
| Acute | Maintenance |
Declination
|
||
Percent |
100 75 50 25 |
|
||
| 0 1 2 3 4 5 10 15 20 25 30 35 40 | ||||
Post Injury (Years) |
||||
Model of Aging and Physical Disability |
||||
The second, or maintenance, phase is best illustrated by the majority of the spinal-cord-injured population. Members of this group, as a rule, are continuing at the level of function they attained following their injury. For the most part, few new problems or needs are arising.
Finally, the first or acute restoration phase is best illustrated by the traumatic head injury population. Within this population the optimal treatment programs to restore function are still evolving.
Although the SCI and traumatic head injury groups are still in the early stages of the model, it can be predicted that each will move through the successive stages and have their own patterns of decline.
Utilizing this model, as well as the previously discussed overlapping developmental spheres of the aging process, it is possible to understand how each individual will have a unique pattern of aging based upon physiologic age, societal interaction, self-realization, anatomic or neurologic level of injury, and the length of time post-injury.
CHANGING MODELS OF CARE
At the beginning of this chapter, it was noted that the medical model of care has been the guiding force of systems of SCI care from the beginning to the present. Multiple forces are at work changing this. An increased awareness and responsiveness to ethics has challenged the paternalistic (medical) model of care as desirable or acceptable for chronic illness. The Hastings Center for Bioethical studies has authored several major position papers relevant to acute and chronic illness (15,16). Equally important are the influences of recent legislation such as the Americans with Disabilities Act (ADA), signed in 1990, and the influences of independent living programs and other consumer advocacy groups. All demand an increased participation of individuals with disabilities in health care and planning. How systems of care will evolve to meet the changing needs of aging SCI survivors is explored further in Chapters 26 and 30, and the future remains to be seen. Hopefully, the subsequent chapters of this book will expose the reader to some of the many issues involved.
Whatever the tribulations of aging, the term grace is frequently used to explain them. Often, we hear the expression “aging gracefully.” Grace means many things to many people. For many, grace is that state of being which arises out of suffering and adversity. As we move through this book and our experiences with spinal cord injury, may we all sense and realize the grace that can come from it.
REFERENCES - Section #1
Section #2: Changing Care Needs
Frederick M. Maynard, Jr.
As people with and without chronic disabilities, including those with muscle paralysis secondary to spinal cord injury (SCI), become older, many physiologic changes can be expected to occur in the body's organ systems, as described in previous chapters. As a result of these changes and associated impairments, new functional limitations and additional disabilities commonly develop. These types of organic-biological changes demand appropriate alterations in the psychosocial and environmental aspects of a person's life in order to maintain the equilibrium known as “good health” and “adjustment” (1). If care needs are understood to include all activities that must be carried out to maintain good health, including social roles that are critical to psychological health, then those needs will inevitably change as the result of new impairments and functional limitations. The most common new impairments and functional limitations associated with aging that occur among people with chronic motor impairments, particularly those resulting from SCI or paralytic poliomyelitis, will be described in this chapter. From a psychosocial perspective, the alternative explanations available to a person for understanding these age-related losses of functional abilities, the resulting impact of these changes on an individual's care needs, and then options available for responding to them will be explained. Lastly, the impact of the aging process on a person's caregivers will be addressed.
The most frequent new functional limitations seen among people with chronic motor impairments result from two general categories of new impairments: musculoskeletal pain problems that further limit postures and use of limbs, and reduced cardiopulmonary fitness that limits endurance. These new limitations frequently affect locomotor and self-care activities that lead to expanded disability. Among survivors of paralytic poliomyelitis, new muscle weakness, pain, and fatigue resulting in new functional limitations is experienced so frequently after 25-40 years that these symptoms have acquired a clinically descriptive label, “the post-polio syndrome” (2). Considerable research has been possible concerning the age-related problems of these people because so many of them were left with residual paralysis after the large polio epidemics of the 1940s and 1950s. Some important observations derived from an epidemiologic research study on this group that are relevant to the issue of aging with SCI include the following (3):
Based on personal experiences with individuals having long-term SCI and on review of the limited research done on aging with SCI, it is likely that observations on aging polio survivors with muscle paralysis will also apply to people aging with SCI-caused paralysis. Additionally, SCI survivors may experience new impairments of skin, bowel, and bladder function which can further limit their functional independence and produce new disability.
UNDERSTANDING NEW DISABILITY
There are two alternative viewpoints for understanding the development of new functional impairments among people with chronic motor disabilities. They can be viewed by either survivor or health care professional to result from age-related normative changes in organs that can be expected to have characteristic manifestations and functional implications among people with any type of chronic motor impairment. Alternatively, they can be considered to result from condition-specific rates and types of changes in specific organ systems that result in predictable new functional limitations. For example, a person with long-standing moderate leg weakness from paralytic polio who has walked with two crutches for 30 years develops painful arthritis or tendinitis of the shoulders which limits walking and leads to greater arm weakness and more shoulder strain. These strain-induced shoulder problems could be considered to not unexpectedly result from prolonged, high frequency heavy loading of tissues which show normative age-related reduced capacity for heavy loading without strain. Alternatively, one could attribute these shoulder strain problems to the onset of progressive weakening of muscles that is unique to people previously affected by polio, a condition known as post-polio progressive muscular atrophy (4). In this condition there is a progressive degenerative fragmentation of giant motor units that is possibly accelerated by prolonged overuse. Psychological distress may be greater with the latter explanation than the former if one views progressive post-polio muscular atrophy as a new disease with an unpredictable likelihood of rapid progression. Some people, particularly those who are relatively young (e.g. in their early 40s), may be more distressed by an explanation that attributes early aging, rather than a new disease, because the notion of growing old threatens their self-image of vitality and implies acquiring other disability characteristics of older people. For other people, attributing the problem to overuse strain may evoke guilt because of their own role in causing it or anger at health professionals who did not warn them about its future likelihood. Although the true cause of these problems may include both explanations, what may be most important for successful coping is an individual's attribution and/or understanding of the cause.
The problems of chronic overuse and progressive muscle weakening probably are not unique to individuals with a history of polio, as illustrated by the following case history. A healthy and physically active man in his early 40s with a 25-year history of C7 quadriplegia presented to a SCI clinic complaining of decreasing strength. Initially after his injury, he was unable to extend his elbows, but he gradually developed more arm strength and became independently able to transfer himself onto a variety of surfaces by his second post-injury year, after extensive rehabilitation. He later participated regularly in a variety of vigorous recreational sports and always used a manual wheelchair for mobility. He reported experiencing a slowly progressive loss of strength in his shoulder muscles over several years and was distressed by this because it threatened to change his active and independent lifestyle. On examination, contraction fasciculations were observed and exertional myalgia was re-produced in his pectoralis major muscle. The muscle also showed partial denervation on electromyographic examination. It was concluded that he was experiencing progressive weakness and pain in the high use muscles of his upper limb which only had partial innervations after his SCI. This progressive weakness probably resulted from the vulnerability that all partially denervated muscles which have been used vigorously for many years have for late onset progressive weakness. People with chronic SCI are likely to experience progressive weakening of those muscles with partial innervations, such as those which recovered strength slowly after the acute injury and which are used strenuously.
RESPONDING TO NEW DISABILITY
The individual described in the preceding paragraph faced several difficult questions that are typical for people who are aging with chronic motor impairments:
If one decides to alter the way an activity is performed, it usually requires obtaining new adaptive equipment and developing new skills for using it. Additionally, decisions to use both new equipment and assistance from others usually have major financial implications and these may influence one's choice of a response to the above questions.
The example used previously illustrates the similarity of the problems and choices faced by people with chronic motor impairments who are aging and becoming more functionally limited, whether their original impairments were a result of polio or SCI. The example involved the dilemma of using the upper limbs strenuously to perform important daily activities, but a similar dilemma is faced concerning continued, strenuous use of the lower limbs for ambulation. Many people with incomplete or low level SCI face this dilemma when deciding to continue walking with braces and/or crutches. The need to face this choice typically occurs for people with SCI after having walking for only 5 or 10 years, as compared to many post-polio individuals who have walked for 30 or 40 years before they face this type of choice about continued walking.
Some of the psychological distress precipitated by the need to make these choices relates to a person's expectations about his or her own functional abilities. Perhaps people with chronic SCI are not as surprised by the loss of endurance or development of upper limb overuse problems that may curtail continued ambulation as the people experiencing the late affects of polio. Many post-polio individuals express anger about their perceived lack of “warning” by health professionals that their enhanced functional abilities as a result of surgery or rehabilitative training would probably not endure for their lifetime (5). Based on the experiences of the post-polio population, a general guideline about the long-term prognosis for maintain functional abilities is that those functional activities that required the greatest personal and/or therapeutic effort to achieve are the most likely to be lost as a result of age-related declines in physical capacity. These include such activities as walking without assistive devices, walking independently with devices, transferring independently, feeding and dressing oneself, or breathing without mechanical assistance.
IMPACT OF CHANGES ON CARE NEEDS
There are several life domains of care needs that can be impacted by age-related change in impairments and/or functional limitations. At the most basic level is what is commonly known as a self-care domain. This includes eating, dressing, bathing, grooming, and toileting. The ability to perform each of these activities independently may depend on the use of specialized equipment and/or on complex skills requiring peak performance of several organ systems. In addition to these normative self-care activities, people with SCI often have many additionally activities that must be done daily or regularly to maintain their health. Examples include thorough skin inspection, especially of bony prominences and old scars; joint range of motion and muscle stretching exercises; breathing exercises; and specialized procedures to initiate elimination of urine or stool. Even if people with high-level SCUI never gained the ability to do these activities without assistance, they probably needed to learn how to assure that the proper performance of these activities was done by others and how to evaluate results in order to make appropriate modifications in their performance.
In a recent study of aging and SCI (6), health status was found to decline related to years post-onset, but not chronological age. Since the oldest age group was under 60, it can be expected that older people with SCI, particularly if they are greater than 20 years post-onset, will experience declines in general health. Therefore, as a person with SCI ages, both chronologically and by accumulated years post onset, the likelihood of complications in the organ systems typically impaired by SCI, and made vulnerable to complications since the onset of SCI, will increase. Many medical complications of the skin, respiratory, gastrointestinal, genitourinary, and musculoskeletal systems will necessitate a change in the previously performed routines for managing the physiology of these organ systems that are altered as a result of SCI. New routines often create a need for new skill development, new equipment, and/or additional assistance from others. For example, an older person may have to begin using suppositories or catheter equipment which may be impossible to use independently. A similar problem can result from the onset of co-morbidities. For example, a person with quadriplegia may develop diabetes mellitus that requires insulin injections that cannot be self-administered. Another example is the development of glaucoma that requires the use of eye drops that cannot be done independently or that severely reduces the visual acuity of a person with quadriplegia.
A particularly difficult choice occurs for people with SCI who develop new impairments which limit their participation in previously routine aerobic activities, e.g. long distance wheelchair pushing or wheelchair basketball. Cessation of these activities in order to remedy an upper limb strain problem may lead to reduced endurance that affects job performance, as it might for a non-disabled person. Balancing the implications of altering, stopping, or acquiring help for specific activities may become a recurrent challenge for people with SCI who have become accustomed to living near the limit of their maximum physical capacity.
Another life domain of care needs impacted by physical changes is homemaking, that is, activities required to maintain a residence, such as food preparation, cleaning, shopping, and yard work. Many of these activities are often shared among residents of the same household by non-0disabled people. New functional limitations may require renegotiation of homemaking responsibilities, or consideration of additional assistance from others to have them completed. A critical activity for independent lifestyles and for life satisfaction is community mobility. The ability to negotiate distances in one's community and access transportation services (public or private) that are needed for essential homemaking activities in most American communities is vitally important. New limitations in endurance commonly impact this important area and require changes in previous routines. Whereas there are many readily available technological choices for maintaining independent community mobility in the presence of severe endurance restrictions, most are expensive and cumbersome, such as electric wheelchairs that require powered lifts on private or public vehicles.
A third life domain of care needs frequently impacted by physical changes is performance of activities that are part of social roles. These may include family roles such as parent, sexual partner, decision maker, or friend; vocational roles, including paid and volunteer activities; or roles involving friendships and leisure time use. Changes in functional abilities resulting from new impairments often precipitate reexamination of personal choices to participate in role-related activities in the same way or to the same degree. New assistance from equipment or other people may be needed to permit continued role-required behaviors. Some roles may need to be given up or redefined. Decisions involving continued full-time employment can be particularly difficult because of their major impact on financial status and/or life satisfaction. Chronological age is likely to have a large influence on these decisions since it affects personal role expectations. For example, a man who was a hospital administrator sustained a C6 quadriplegia at age 39. He continued working part-time throughout most of his initial rehabilitation stay at the same medical center where he was employed. He returned to his demanding 60+ hr/week job within 6 months after his injury, and maintained his family roles, which included parent and spouse. After only 7 years with this very physically demanding lifestyle, he reluctantly decided to retire because he could not maintain the demands of his full-time work without a variety of stress and exhaustion-related symptoms, and because financial disincentives were too great for part-time or alternative work. Perhaps his decision would have come sooner and been somewhat easier if his current age was 56 and not 46.
OPTIONS FOR RESPONDING TO CHANGES
There are basically three types of options available for responding to changing care needs that may result from new age-related impairments and functional limitations:
Attitude is another critical change which is necessary for optimally adapting to new age-related impairments and functional limitations. The most difficult readjustment for some individuals is in their style of coping with functional limitations. For example, a person with polio who struggled long and hard in the past to be able to walk may find it difficult to accept the use of a wheelchair for community mobility. Similarly, a person whose fight to achieve independence in daily living skills was one of his or her most important life accomplishments may be intensely distressed by the need to accept assistance from others, even if money and availability are not problematic. Among people with the late effects of polio who have been severely disabled for many years, it has been observed that when their freedom to control life activities is threatened by new physical limitations, or even by temporary dependency imposed by a hospital setting, they may experience a threat to their whole life and purpose for living. This reaction often leaves them vulnerable to other's false perceptions of them as being overly controlling, difficult, and demanding people. In reality, it might be more helpful to consider them as simply knowing what they need and being not too timid to ask for it. Informed health care professionals and caregivers will accept their behavior as adaptive and do everything possible to let them feel and actually be in charge of what happens to them (7). These same reactions can be observed in people with chronic SCI. It may be helpful to point out to them that by relinquishing their struggle for physical independence and accepting new personal and technological assistance, they can gain the time and energy to develop new pursuits and cultivate other realms of interest. Mental and behavioral flexibility, including reframing the half empty glass into the half full glass, may be the most important characteristic for maintaining an acceptable quality of life as one ages and experiences progressive disabilities.
Based on a conference of people with chronic SCI (8), and with people experiencing the late effects of polio (7), the most frequent attitudinal and behavioral change needed in order to successfully cope with new impairments and functional limitations can be summarized as slowing down and adopting energy saving techniques. The philosophy for approaching life with a physical disability that is known as “use it or lose it” must be replaced with a “conserve it to preserve it” approach. People in a declining phase of physical capabilities need to adopt energy saving techniques for performing important life activities, such as using a “reacher” rather than straining shoulders for reaching high objects or using an electric wheelchair rather than pushing a manual one to negotiate the distances of a shopping mall. Making this midlife-with-disability attitudinal change allows an individual to reconsider the quality and quantity of health problem prevention activities that are routinely performed. The method used for skin pressure relief, the type of protective sitting cushion, the frequency of urological evaluations or nutritional habits may all need to be reexamined seriously during the stage of life when new impairments and functional limitations begin to be recognized and new care needs develop.
IMPACT OF AGING ON CAREGIVERS
Changing care needs accompanying aging not only affect the individual with chronic disability; they also affect their supportive network of other people. New problems from the impact of aging on caregivers are most likely to develop among those people with SCI who have needed assistance from others for personal care and homemaking services since the onset of their SCI. A recent survey of arrangements for receiving personal assistance services among people with SCI found that 50% received assistance exclusively from family and another 19% received some services from family. Living with and receiving assistance from family members was the most common living arrangement among this SCI population (9). As pointed out by Trieschmann, women most often take on caregiver roles in families, and the burdens of assisting family members with disability most often falls on wives, mothers, and daughters (1). Due to the predominant male demographics of SCI, most spouses of people with SCI are wives. The primary advantage of family caregivers is low cost, although quality and reliability of services are also rated high (9). Disadvantages of family caregivers included low dignity and control, including the special psychological burden of adult children being cared for and not living independently of parents, which can stunt the development of self-confidence and esteem. This living arrangement may also interfere with the fulfillment of noncaregiver family roles. For example, it may be difficult for a husband with SCI to remain a desirable sexual partner for his wife is she also carries out his routine bowel program.
In addition to routine physical assistance the contribution of family members to a disabled individual by providing emotional support must be emphasized. A network of friends, that may include family, is usually vitally important for back up provision of personal care services in the event of unexpected no availability of paid personnel.
With passing years the possibility at age-related changes among caregivers will occur and affect a person's lifestyle becomes greater. Indirect effects of aging on caregivers can result from the increased needs for assistance that age-related changes in the care needs of persons with SCI bring. However, age-related changes often occur concurrently in the very caregivers that may be asked to take on greater responsibilities. For example, a spouse may develop arthritis that prevents her from continuing to assist with transfers, particularly as transfers of a weaker and heavier spouse become more difficult.
A second problem among long-acting caregivers is “burn-out,” which is the condition of becoming unable to continue coping with chronic physical and emotional stress resulting from long-held responsibilities. While little research on burnout among caregivers of people with chronic disabilities has been conducted, few doubt that it occurs. A study by Schultz and Wood assessed factors associated with psychological well-being among 67 caregivers of people with SCI (10). They found that high levels of psychological well-being were associated with their own good health, high levels of perceived control, the feeling that they received adequate social support, and their satisfaction with the quality and quantity of social contacts. Depression was correlated with the amount of assistance they needed to provide. In another study of parents with ventilator-assisted children, it was found that the most stressed parents were those with the fewest resources for coping with stress (11). The amount of care actually required was unrelated to signs of stress. Parents who coped well also received support from their own families. These findings emphasize the importance for health care professionals of discussing the impact of age-related increased care needs on routine caregivers. People with chronic SCI may need professional counseling concerning how to communicate these concerns with family caregivers and/or how to problem-solve alternative options for meeting care needs. The concept of respite care derives from culturally defined expectations of family members providing care to aged parents or children. Respite care is a good idea for all caregivers in order to avoid burnout.
All support systems will eventually change and nondisabled spouses or caregivers may die or become disabled themselves before the death of a person with chronic SCI. Therefore contingency planning for meeting personal care needs is important. Financial resources always remain the primary issue when discussing changing care needs and contingency planning. Worry about money can strongly influence the perceived burden of care by family caregivers. Experience with post-polio individuals in the 40-50 age group, most of whom have had higher education and well-paying jobs, indicates a high interest in learning about the complexities of Social Security regulations concerning early disability retirement and survivor benefits (12). Planning for life in environments with few physical demands and with ready availability of assistance services relating to disability is a pre-occupation for many able-bodied people as they approach or enter retirement years. Clearly there is a need for special attention to the topic of older life financial security planning for people who are aging with chronic SCI.
In the United States, there are too few options beside nursing home residence for people who need assistance with personal care needs but have no family members to provide it. Traditional nursing homes are generally considered the worst possible alternative for residence by most survivors of chronic SCI, many of whom may have had previous personal experience with living in them. Such residential alternatives as cooperative or supportive living is clustered housing have been shown, particularly in Europe, to offer many financial and social advantages (123). Unfortunately, they are very expensive and rarely available in this country. Home health services are widely available and can meet short-term needs that might arise for some older individuals with chronic SCI. However, for routine personal care services, they are almost always too expensive for payment using private monies and are not a benefit of most insurance plans. The role of centers for independent living (CILs)) in assisting people who have aged with chronic SCI in obtaining affordable assistance services and/or alternative residential arrangements has not been fully explored. Probably the same services and methods used for people who are recently disabled would be adequate with few alterations. Greater dissemination of information about the services of CILs to older people with chronic SCI is needed because many of these people are unaware of CILs and their services. Consumer-based advocacy and service organizations did not exist during the era when most people with SCI for more than 20 years were first rehabilitated. These survivors may need detailed explanations about the potential ways that these organizations may assist with enabling people with disabilities to retain their psychological independence and autonomy in spite of increased physical dependence.
CONCLUSIONS
As people with chronic SCI age, they become increasingly likely to experience new impairments and functional limitations that can increase their disability. The experience of people with long-term muscle weakness from paralytic polio illustrates the propensity to overuse related musculoskeletal problems of the upper limbs associated with leg paralysis. The wide variety of new health problems that may be unrelated or related to chronic SCI creates the need to make difficult choices about how to best cope with changing care needs. Changes may impact self-care, homemaking, work, or leisure activities and roles. Options for responding to changes include acquiring new skills, using new equipment, utilizing assistance services from other people, altering priorities for customary activities, and/or changing attitudes. Approaching physical challenges with a “use it or lose it” attitude should be replaced by a “conserve it to preserve it” philosophy. Changing care needs also have an effect on caregivers. Lifetime care plans to deal with unexpected losses of caregivers and strategies to prevent burnout of caregivers are needed. Re-rehabilitation and independent living services are likely to be needed by people who develop increased disability from age-related changes in care needs in order to preserve their autonomy and quality of life.
REFERENCES - Section #2
Section #3: Psychological Adaptation
Lester Butt & Melinda Fitting
Little is known about how people with spinal cord injuries (SCI) psychologically cope with their injuries as they grow older and are faced with the complexities of the aging process. There is no one response to the changes wrought by the aging process, and, in fact, people become more heterogeneous as a group as they age. As a result, there is even greater variety in the older years than in the younger. How a person with SCI copes with the “normal” changes in one's life that occur in the middle and older years is most probably the result of a multitude of factors. Some of these factors will be addressed in this chapter as well as a discussion of several salient clinical issues facing rehabilitation specialists.
Rubenfeld, in her article, “Ageism and Disabilityism: Double Jeopardy,” speaks to the psychological impact of these multiple issues. Addressing disability, she holds that disability has been viewed as the product of evil possession – persons with disabilities are consequently seen as objects to be “ostracized, feared, devalued, or (at best) ignored” (1). Present day manifestations of these primitive beliefs involve the conception that people with disabilities should be institutionalized for life, and defined “in terms of our condition rather than in terms of who we are.” Similarly, speaking to the issue of ageism, Rubenfeld holds that “Ageism discriminates against the old with inaccurate and misleading stereotypes, just as racism and sexism discriminate against skin color and gender, and just as disabilityism on the basis of physique. Old people are seen as senile, rigid in thought and manner, garrulous, and old-fashioned” (1). Robert Butler, the first director of the National Institute for Aging, believes that the etiology of ageism stems from a multiplicity of cultural influences, ranging from social pressures to produce commodities to a thinly disguised attempt to avoid the realities of aging and death (2).
It may well be that persons with a disability deal with issues of prejudice in a different order than the nondisabled population – in other words, they become disabled and then age while the rest of the world ages and then deals with disabilities. Aging challenges us all with the physical changes in our bodies, the losses of status and income, the increasing need for assistance as we become more frail, the psychological issues of death and loss of family and friends, and the normal cognitive changes which accompany the aging process. Aging is a great challenge to all of our resources and what we lack most is a clinical knowledge base specifically describing how people with disabilities differ from nondisabled people in this process.
The specific focus in this chapter revolves around the psychological adaptation to the developmental issues of aging and the interaction with increased duration of time post SCI. Toward this goal, the following areas will be addressed:
CRISIS THEORY
The advent of SCI is usually traumatic, and as such, extratemporal in nature. However, some explanation of the concepts of stress and crisis are in order to appreciate the area of adaptation. Crisis theory is based upon the notion of homeostatic balance, with the assumption that the individual is normally within a state of relative equilibrium. During a lifetime, people learn adaptive coping mechanisms which allow them relative success in resolving problems. Typically, individuals are able to cope with unusual and difficult concerns without accompanying frustration that reaches an incapacitating level. Coping skills allow for the tolerance of frustration, the creative resolution of problems, and the discharge of accumulated tension. This process maintains or restores equilibrium in the face of life's obstacles.
A crisis occurs when “a person faces an obstacle to important life goals, that is for a time, insurmountable through the utilization of customary methods of problem solving. A period of disorganization ensures, a period of upset during which many abortive attempts at solution are made” (3). Crisis, then, is an upset in the steady state. The relative state of equilibrium, involving a system which links family, society, and individual, has failed in its adaptive maneuvers and problem-solving efforts.
Crisis is emergency plus a sense of incapacity. Emergencies may be handled by self-assured action whereas crisis involves the emergency variable without prescribed and effective methods of coping. A person is much more likely to handle a stressful situation adequately if it has been heretofore successfully managed. Conversely, failure to cope with a particular problem lends greater vulnerability to the issue when next encountered, in that the psychological residuals of failure and demoralization remain. Coping and adaptation can be defined as any response to external life strains that serves to prevent, avoid, or control emotional (and cognitive) distress. Schwartz provides analogies to the concept that crises occur in relation to the extent to which individuals have learned to handle the situations with which they are confronted (4).
Each successfully managed hazard or crisis can add to the coping armamentarium. Exposure to a crisis situation, then, can be said to either enhance the repertoire of responses or to reinforce maladaptive methods of coping.
Several different types of crises may emerge during a person's life. Some crises occur as part of a stage of life, such as adolescence, middle age, and old age. Assuredly, there are inherent transitions within the aging process itself. In contrast with this type of crisis are those which occur when the person is pushed to the next developmental stage, with is accompanying stresses and learning demands. Examples include marriage, parenthood, and promotion at work.
In addition, a third category of crisis is extraemporal, occurring independently of time of life. This is the type of crisis brought on by traumatic accident, such as that resulting in SCI.
Clearly, the initial impact of life with a traumatic SCI is met with stress and potential crisis. However, as a tribute to the human spirit, most individuals respond with eventual accommodation and adaptation. The question remains as to the long-term pressures on one's adaptive abilities as one ages with inherent, additional stressors. Assuredly, there are multiple sources of stress, reflected by the interaction of spinal injury with the aging process.
ACUTE AND CHRONIC ILLNESS AND DISABILITY
In order to appreciate psychological aspects of the self, it is imperative to differentiate between acute and chronic aspects of disability. Appreciating chronic disability mandates an understanding of the manner in which it impacts the individual, the family, the individual's social matrix, and the general health care system. Certainly, an appreciation of chronic disease is only one aspect of the total reality of chronic disability. The manner in which practitioners conceptualize acute, self-limiting and infectious diseases is far from adequate for the understanding or response to the personal, social, and bioethical challenges of chronic disability. Chronic disability, by definition, lasts for a substantial period of time or has sequelae that are debilitating for a long period of time. It commonly interferes with daily functioning for more than three months in a year, causes hospitalization for 30 days or more per year, or (at time of diagnosis) is likely to do either of these. The goal of medical management of chronic disability is not “cure” in that the condition cannot be completely reversed or compensated for. The impact of chronic disability is transformational in nature, in that it affects personal and social arenas. Commonly, persons with chronic disabilities experience restricted activity, dependency, and interference with vocational pursuits and economic security. Additionally, there is the potential associated stigma of intolerance, fear, and misunderstanding or patronizing sympathy. Persons with chronic disability strive toward maintenance of personal dignity and respect for themselves and their families (5).
The impact of a chronic disability upon an individual's self-image can be constructive and/or deleterious. This experience has been labeled both enabling, one that enhances an individual's abilities and resiliency, as well as stigmatizing, alienating, and isolating, leaving the individual without purpose and future direction. Yet the relationship between chronic disability and self-identify is far from static. There is a multiplicity of issues that impacts this equation, including current symptoms of the disability, reaction of family, friends, and caregivers, and the various adaptive gambits individuals utilize.
Chronic disability raises exceedingly complex philosophical questions about the nature of the self and the continuity–or discontinuity–of self-identity over time amid changes in organic capacity, social circumstances, and in the ability to actively shape and direct one's life. Is the self an entity that stands above and apart from the body and the social persona so that even drastic changes in body or persona leave the essential identify of the self unchanged? Or, at the other extreme, is the self so constituted by the organic condition of the body and external social perceptions, that in the face of progressively debilitating and disabling chronic disability it may be said to have no essential stability at all? (5)
The issue of personality stability over time will be subsequently explored via available empirical research.
In contrast to acute medical care, chronic disability does not involve complex invasive and sophisticated technology. Usually, chronic care is provided on an outpatient basis wherein patient compliance is essential. Additionally, the conceptualization of illness is markedly different in acute and chronic illness/disability. Within the acute illness model, the illness is viewed as an “alien threat to the self, and the goal is to defend and restore the self by curing or compensating for the illness” (5). The illness is viewed as inherently evil and dystonic to one's being. According to the acute illness model, the provider and patient enter into a contract wherein the goal is to defeat the illness enemy. Restoration of functioning to premorbid status is the aim, via destruction of the enemy within to eventuate a cure. Inherent within the acute medical model is the traditional doctor-patient relationship, wherein the patient's role is typically passive in nature.
However, the vision of chronic disability is indeed a counterpoint to the aforementioned conceptualization of acute care. Chronic disability is not reversible, nor a transient aberration from one's premorbid life. Indeed, chronic disability mandates that its sequalae be integrated into the essence of one's being. Accommodation to, not elimination of, the disability state is paramount. Chronic disability care is therefore directed towards the minimization of the impact of the disease/disability process.
In the face of chronic illness the paramount good that medicine should serve is not precisely health – at least not ideal health, which is a chimera in any case – but rather the wholeness and the integrity of the self. Persons with chronic disability really have no choice but to try to integrate their disability constructively into their daily lives and sense of self-identity. The desideratum is to stay intact–to make the necessary adjustments with as little loss of purpose, coherence, and meaning in life as possible . . . Living with chronic disability is thus a process of negotiation . . . Whereas acute care aims to restore one's freedom from illness, the goal of chronic care is to sustain meaning in life with–and in spite of–illness. Diplomacy is perhaps a better metaphor than warfare for this kind of care. Medicine's role in chronic care is to facilitate the process of negotiation. (5).
One cannot dichotomize oneself from the chronic disability; indeed, one needs to eventually reconcile and integrate aspects of the chronic disability into one's self-concept. As such, the accommodation to chronic disability is a biographical event, in that it is highly phenomenological in nature. Therefore, there is no one path to a positive outcome, but rather diversity as vast as permutations of personality.
This view of chronic disability is consonant with the view of accommodation to aging and the changes which can occur. At 75 years of age most people have a chronic disability to which they are accommodating their lives, but they are not disabled per se. These chronic disabilities may be heart problems, arthritis, hearing and vision problems, or they may be serious cognitive disorders such as Alzheimer's disease. People respond to the same limitation, such as heart disease, quite differently, with some people exhibiting “excessive disability” and restricting their lives more than their underlying condition warrants, while others proceed with their lives in a vital manner with the least restrictions possible.
Disability at any age affects people in diverse ways. However, there are commonalities in spite of the wide array of styles. Murphy, himself disabled, writes:
Disability is not simply a physical affair for us, it is our ontology, a condition of our being in the world . . . My identify has lost its stable moorings and has become contingent on a physical flaw . . . Paralysis is an allegory of life and entropy, and my search for their relationship places me in the role of the shaman, who seeks to reconcile the sick person to his illness by placing it in the context of timeless myth and belief....My task differs from the shaman's in that is seeks no cure, only comprehension. (6).
The chronic disability provides the framework upon which value and meaning are constructed.
Erickson's personality theory is relevant to people with spinal cord injuries who know are facing the aging process. Specifically, Erickson's theory is sequential, sociohistorical, and dialectical in nature (7). The dialectical aspects of Erickson's developmental personality theory mesh well with the previously mentioned inherently constructive and destructive aspects of disability. Assuredly, the presence and spectre of chronic disability is a crisis, and demands that one changes, adapts, and modifies oneself. Erickson conceptualized that as one ages, one contends with the dialectical issues of identity versus role confusion in the adolescent years, intimacy versus isolation in early adulthood, generativity versus stagnation in the middle years, and ego integrity versus despair in the later years (7). Chronic disability can bring new growth and psychological change as one confronts one's limitations and opens oneself to new possibilities. Consequently, the individual with chronic disability is confronted and contends with the dialectical extremes of self-rejection and self-love, withdrawal and participation, dependency and autonomy, mourning and celebration.
While there is a dearth of research superficially on SCI and aging, there is relevant empirical research that bears upon chronic disability and coping/adaptation. Specifically, these areas include personality stability and psychopathology across the lifespan, the nature of coping and gender differences.
Far too often, theorists and researchers of coping/adaptation have focused upon the specific time frames and, therefore, not conceptualized in longitudinal terms. However, this is not the case within the gerontological literature, where coping and adaptation is viewed from a psychological/developmental perspective. The three theories of psychological adaptation that will be explored are the
PERSONALITY THEORY AND STABILITY
A conception that is intrinsically involved with adaptation and aging revolves around the complex issue of personality. A commonly held assumption is that with aging there are inevitable, concomitant personality changes. However, this is a myth surrounding the aging process. Heterogeneity and variety are more common in the later years of life than in the younger. This makes intuitive sense in that there are more life experiences and more permutations possible as individuals age and change throughout their lifetimes. Each individual grows older in his or her own unique way, even though there may be similarities and cohort effects.
Research by Costa and McCrae suggests that personality is stable over the lifespan (8). They have researched traits which they have classified into five domains representing a full range of personality variables. These domains include neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness. Older people did not differ from younger people substantially on the researched traits. Longitudinal data are also suggestive of the hypothesis that personality characteristics are stable over time. For example, people who were open in their younger years tend to be open in their older years. People who were rigid when they were 25 will be rigid when they are 85.
Another developmentalist, Neugarten, has posed the concept of timing of events in the lifespan (9). We expect certain things to happen at certain times; examples include finishing school, marrying, bearing children, retiring. When events are nontemporal such as a chronic illness/disability (SCI at age 20 rather than disability at 75), they may prove more difficult with which to cope. People expect chronic illness when they are in their 70s; however, SCI is typically an unexpected event at any age.
Men and women may relate to aging with a SCI quite differently. The psychological issues of independence and autonomy are important to all of our lives throughout our lifespan. As people age they usually are forced to struggle with some diminishment of autonomy and control over their environment. In one's 80s we see a group that is referred to as the “old-old” who simply become more frail and need more assistance with their daily lives. For those people who are victims of dementia, we see individuals adjust to the cognitive changes over which they have no control and the diminishment of autonomy given these cognitive changes.
There are no clear gender differences as people age and cope with the physical and cognitive changes with the concomitant increase in dependence; rather, it may be that personality is the most salient feature. People who like to be in charge and rigidly control their lives may struggle the hardest with the dependency as they age. Rodin suggests that medical personnel would be wise to be attentive to these differences in control when designing treatment strategies, because when options are congruent with the control style of the patient, the psychological and physical accommodation is enhanced (10). Men have been socialized to be more in control than women and this may have an impact on the dynamic between independence and dependence. Women have been socialized to view themselves as interdependent and may allow themselves to accept the help needed as their physical abilities change due to the aging process. Men, on the other hand, may exhibit more difficulty accepting the fact that they need more assistance and may resist this as antithetical to their self-concept.
This issue of independence and dependence is a crucial dynamic in our culture and has a ubiquitous affect whether one has a disability or not. SCI will affect the equilibrium between these two poles as will the aging process. Do men who sustain spinal cord injuries in their early years learn how to cope with dependency issues more effectively than men who are faced with these issues much later in life? Do women cope with the dependency issues as women with spinal cord injuries better than their nondisabled counterparts in later years? These issues have yet to be empirically explored.
There are clearer patterns of gender differences in elderly caregivers. Traditionally women have been the caregivers for children and for ill or disabled family members. Traditionally, men have more been the ones who worked outside the home and did not provide much hands-on caregiving for others. One theory postulated that while women become more interested in the world outside the home in the middle years, men at the same ages become more interested in the family relationships and the home (11). It is as if their life trajectories cross over one another as opposed to being parallel. For people with SCI, it may be that spousal or parental female caregivers may not be able to sustain this role as the person with SCI ages. They may become exhausted by the role or, if they are elderly parents, may be faced with their own chronic illnesses. Male caregivers may look at caregiving as a new job if they have not been providing care before, and may, therefore, not be depleted by its occurrence in the middle years.
DEVELOPMENTAL MODELS
In order to appreciate the issue of adaptation over a life span, it is necessary to focus upon several developmental models: the “life events” model, the “cognitive appraisal” model, and “subjective well-being” model, and the “psychological lifespan construct” model.
The life events model of adaptation is predicated upon the aforementioned concept of homoestasis. Herein, all individuals strive towards the state of homeostasis; life events that disrupt homeostasis are crises in that they require resources of time and energy prior to return to steady state. Holmes and Masuda hold that stress is assumed to be a mediator between an event and adaptation to the event, causing damage to physical and psychological systems the longer and more intense the disruption of the individual's usual life patterns (12).
Within the life events model, the individual's response to a life change is increasingly being understood as a function of personal and social resources at the time the event occurs. These personal variables include:
Social resources include age, education, occupation, and income. Most accurately, it is important to balance between one's assets and liabilities for this calculus to illustrate the highest degree of validity. Coping, the individual's attempt to restore homeostasis, involves securing information about the adaptation requirements posed by the stressful event. Janis holds that coping involves appraising the range of alternative actions, reaching a tentative behavioral plan, acting on this plan, and then adhering to it (13). McGrath believes that coping also may involve taking actions that prevent the stressful event, prepare for it through anticipating its impact before it happens, rehearse ways of dealing with it if it does happen, or minimize its importance as a threat (14). This is in contrast to avoidance, which most often is construed as defensive and negative in nature. Consequently, the life event, SCI and its sequelae, creates discord via the inherent stress that requires change in life. Stress is regarded as the degree of readjustment necessitated by the event. Coping strategies are employed in order to contend with the stressful life event.
In summary, the major flaw in this theory of adaptation is via its exclusive attention to observable events, the subjective nature of the SCI and its perceived consequences are lost. For example, the connotative meaning of the spinal injury whether its signifies abandonment, loss of self-control, threat to masculinity or femininity, punishment for worthlessness, fears of loss of autonomy or perfectionism, threat of intrusion, and/or fear of attack-is not mentioned.
As with the aforementioned control style issue described by Rodin (10) the rehabilitation staff needs to be sensitive to the interaction between the SCI and its connotative meaning to the individual.
An alternative to the life event model is the cognitive appraisal model. In this conceptualization, the realm of subjectivity is given the greatest play. Lazarus holds that stress is not solely a mediator between the event and the individual reaction to that event, but also is envisioned as the outcome of the event, the stimulator of subsequent reactions, and the result of these reactions (15). This model is subjective in that it is the result of attempts by the individual to interpret situations and then to deal with the requirements generated by the interpretation. This leads, in turn, to reinterpretations of the significance of the event.
Lazarus describes this framework as “cognitive-phenomenological.” This means that the way in which the individual appraises his or her relationship with the environment determines the emotional reaction to the environment. An appraisal is a judgment of the significance of the event to well-being. The appraisal process is seen as a function of motivational constructs such as beliefs, goals, and values; such constructs, along with learning, memory, and perception, are labeled “cognitive” (15,16). Further discriminations are differentiated into primary and secondary appraisal. Primary appraisal is the evaluation of the significance of an event for its impact or possible impact on well-being. This evaluation characterizes the event as either irrelevant, benign or positive, or stressful. The evaluation of stressful does not necessarily imply threat, but may alternatively imply a challenge or opportunity for growth. The primary appraisal also determines the affective/emotional reaction to the event, ranging from anxiety fear, anger, guilt, to joy, hope, or excitement, contingent upon the specific interpretation of the situation.
The appraisal of a situation as threatening or challenging is also a function of the individual's perception of his or her own capabilities for meeting its demands. This evaluation constitutes the basis for the secondary appraisal process. Secondary appraisal involves evaluation of what personal and social resources are available, how well a particular mode of coping will meet the situational demands, and the “costs” of that coping, that is, whether new problems will result from the actions taken to reduce the threat or meet the challenge. Secondary appraisal is influenced by personal motivations and skills and the situational indicators of harm or gain that are mediated by the primary appraisal. This process is highly dynamic in nature, providing a consistent feedback loop to the individual regarding the revised interpretation of the event subsequent to evaluation of the event as well as one's perceived abilities. Herein, coping refers to the actions taken by the individual to reduce a stressful situation or act upon a challenging opportunity. Coping can serve two functions: an instrumental function which changes the nature of the person-environment relationship, or a palliative function which is served when the nature of the person's emotional reaction to the situation is improved (17). Consequently, this model avoids two liabilities of the life event schema, in that the cognitive appraisal model appreciates the individual's interpretation of the event as well as the utilized coping strategy that is contingent upon the event's idiosyncratic interpretation. Importantly, this model takes into account the dynamic, changing view of self and the world.
Lastly, one needs to consider Whitbourne's psychological construction of the life span, which provides the inclusion of the best aspects of each of the above (18). The lifespan construct is viewed as a unified sense of past, present, and future events linked by their common occurrence to the individual. It is both cognitive and affective in its scope. Whitbourne holds that the lifespan construct develops transactionally with identity, changing identity as it, itself, is changed. There are two components of the lifespan construct: the “scenario” and the “life story.” The scenario consists of expectations regarding the future. It is “the translation of the lifespan construction into such plans for the future in the area or areas that have been defined by identity as important” (18). The scenario is strongly influenced by age norms that define the transition points and associated “acceptable” ages for making these transitions. “As the individual begins to advance into the positions defined by the scenario, it will inevitably be revised. These revisions may be purposeful, taking place as the result of planned change, or inadvertent, as the outcome of unexpected intrusions from the outside world.
At the same time, the individual begins to build the “life story,” which is the second manifestation of the lifespan construct (19). The life story incorporates past events into an organized sequence, giving them a personal meaning and a sense of continuity” (18). This provides an organizing principle of all life experiences. In this framework, the content of the lifespan construct determines the content, level, and timing of one's aspirations, which in turn provides the basis for appraisal of event significance. Coping may result in an altered life story so that the meaning of events is distorted according to one's biases toward the maintenance of self-esteem. Coping may also result in altered aspiration levels though any revision of the lifespan construct involving a changed scenario. This can involve a restructuring of identity in response to a real need to make changes in one's estimation of one's capacities toward greater congruence with one's actual competencies. Consequently, the motivation for identity restructuring is not simply self-esteem maintenance; rather it is the desire to solve everyday problems more effectively.
The adaptation process takes on different configurations dependent upon whether the event is consistent or inconsistent with the individual's scenario. For example, an event consistent with the scenario is evaluated favorably and is integrated into the individual's life story, and serves as further confirmation of the scenario. This integration, however, does not necessarily imply that the integration will have a positive impact; indeed, it may have an upsetting affect. The issue at hand is its consistency with the established scenario. Yet what happens to an individual who experiences an event that is inconsistent with one's scenario?
The first possibility if this occurs is for the individual to incorporate the event in a fairly accurate manner, in spite of the very nature of the event's inconsistency with the scenario. As a result, identify is altered, which in turn modifies the lifespan construct, and results in a revised scenario. Subsequent life experiences then are evaluated in accord with this newly revised scenario.
A second possibility exists when the life event is distorted in order to provide consistency with the scenario. Herein, no new insights regarding identity or an alteration of the lifespan construct will occur. Consequently, this cognitive maneuver involves ignoral and distortion.
Lastly, the individual who experiences a scenario-inconsistent event may abandon the environment that provides this feedback. Environmental modifications might not be undertaken until previous attempts are found to be impossible within the context of that environment. Again, no new alteration in identity will occur with this gambit. Whitbourne states,
If the event was not only unprepared for but not even a part of the original scenario, the individual will be forced to incorporate it in the scenario as well as make it a part of the life story. This double strain would account for the fact that unanticipated events require greater adaptive efforts on the part of the individual than events that occur before their time but were expected to happen eventually. (18)
Thus, the individual's perception of an event is a function of the structure imposed on it from identity through the lifespan construct and cannot be predicted from a categorization system based on external criteria defined by an observer. Only through the individual can the potential for developmental change be activated.
PSYCHOPATHOLOGY
An important issue to consider when one contends with the topic of long-term adaptation to SCI is age-related psychopathology. There exists the commonly held misconception that higher levels of psychopathology, especially depression, are manifest within the nondisabled, aging population. The thinking behind this position deals with both the assumption of reduced internal coping capacities as one ages, as well as the increased presence of multiple losses that predictably occur. Following this line of thinking, the existence of SCI would stress the internal resources and coping abilities of the individual even more, especially if the injury occurred in later life.
However, there is an alternative hypothesis that SCI later in life may be adjusted to more easily because persons have learned various coping skills throughout their lives that they now apply to this new life crisis. In contrast to the aforementioned belief that there is a higher incidence of major depression within the older population, several studies illustrate a lower incidence rate within the elderly as compared to younger adults (20-23). Several hypotheses can explain this discrepancy: higher incidence of atypical depressive symptoms in the elderly, camouflage of concurrent medical illness, socioeconomic stressors, or inadequate diagnostic and epidemiologic sampling techniques (24-27).
Another hypothesis is that there is a higher incidence of depression in the middle years because there are more stressors in these years with work and family obligations. Mortality is more of a concern in one's 40s than in one's 80s where people are not concerned with death per se but with lingering illness.
One difference within the area of major depressive events within the elderly population is the higher rate of somatic symptoms, such as abdominal problems, sleep disturbance, lethargy, and constipation.
Dementia, while associated with age, is not a normal aging change and is not experienced by the vast majority of elderly. Lastly, sadness and depressive episodes may emanate from life cycle issues, specifically bereavement, socioeconomic status changes, and physical health deterioration. Murphy found an association between major social difficulties, poor health, or other severe life events and onset of depression within the elderly (28). However, good physical health, higher education, sense of personal control, continued supportive relationships, and adaptive skills have been correlated with more positive adjustment to the inherent stressors in aging. These are the same skills that predict positive adjustment in SCI; therefore, it may be hypothesized that individuals with spinal cord injuries may have some preparation for aging that their nondisabled friends do not possess.
EMPIRICAL RESEARCH
The available empirical data specific to the issue of protracted adaptation to SCI is indeed sparse. Additionally, not only is there a paucity of studies, but only one truly attempts to control for confounding variables (29). Confounding variables that impact post-SCI adjustment include the influences of chronologic age, time since injury, and the social and cultural environment at the time of measurement. In a general sense, most studies point to superior long-term adjustment with younger age at onset (30-33). Additionally, time post-injury has been correlated to acceptance of disability (34), life satisfaction (35), and similarity of actual life to ideal life (36). Globally, the data imply a negative correlation of age with adjustment, particularly age at onset of injury. However, there are individuals who sustained their injuries later in life and adjusted very successfully, in part because they had lived fulfilled lives and had developed skills from coping with other life problems that they then used in order to cope with their latest stressor, the SCI. One simply does not know enough at this point to formulate strong opinions about how older people respond to SCI as a group or as individuals. Krause and Crewe found that activities appeared to be correlated more with chronologic age, whereas medical problems were correlated more with time post-injury (29). Both chronologic age and time post-injury were correlated with life satisfaction and self-rated adjustment. As one would intuitively believe, it was found that older persons are likely to experience less active and less rewarding life after SCI than younger persons. Additionally, sex life satisfaction, overall self-rated adjustment, and predictions of future adjustment also decreased among older cohorts. Contrary to the general downward trends with increasingly older age cohorts, however, satisfaction with living arrangements increased linearly. The number of hours per week spent working and satisfaction with employment also increased from younger to older age cohorts. Whereas chronologic age was generally related to a decline in activity level and to some of the psychologic variables, time since injury was more likely to be associated with enhanced psychologic functioning. Satisfaction with living arrangements, satisfaction with employment, self-rated present adjustment, and the number of hours spent per week working all increased with greater time post-injury. Also, time since injury, unlike age, was strongly correlated with medical stability. The authors found that, in general, the older the individual at the time of injury, the greater the likelihood of poor adjustment in many life areas. Additionally, the research suggests that the most devastating impact of SCI is upon the oldest persons and the persons with the least time since injury. Consequently, the younger the age at injury, the greater the opportunity to adjust to the disability (29).
This research provokes as many questions and interpretations as it answers. Hopefully, this excellent beginning will spur more well-controlled empirical investigations towards a greater understanding of protracted adaptation following SCI.
TREATMENT
The treatment and care of people with chronic disabilities involves several factors. Barnard speaks to three issues considered to be essential regarding the “healing of the damaged self” (37). These include:
Empowerment relates to the provision of autonomy, visibility, and voice to the chronically disabled population. Empowerment entails action on biological, psychological, and social fronts.
Branded as the carriers of life's negatives, the chronically ill are marginalized, and the validity of their inner experience is denied . . . In this more integrated perspective, frailty and strength, autonomy and dependency are dialectical parts of a whole, rather than dichotomies . . . Heightened dependency is a reality for many severely disabled people. The healing response is not to deny dependency but to refrain from exploiting it, and to strive to minimize it without judging it so negatively as to stigmatize persons whose dependencies are irreducible. (37).
Additionally, given that chronic disability does not create total metamorphosis of the personality, the rehabilitation effort is geared towards melding surviving elements of the self to new possibilities. Therefore, the rehabilitative task is not only reconstruction but also retention of the self. The healing task is to make contact with the surviving self and affirm its enduring validity and worth. Lastly, there must be attention to individuality. The shift must be made from treating the person as a patient to the more humane model of treating the patient as a person.
One of the contemporary, understandable difficulties with the hospital rehabilitation model has been the prime focus upon young people, and usually young males. The rehabilitation environment and treatment goals need to be made consonant with the age group being treated. Older people may need to be allowed more time to learn the rehabilitative skills and may need more consideration of their energy level. As such, they may require less vigorous workouts at one time. Few rehabilitation specialists have been trained in aging and there needs to be a focus on training staff about the psychological issues that are part of the normal lifespan development. Allowing older people to be in as much control as possible of their program may be more crucial than for younger patients.
It cannot be overemphasized that disabilities affect family systems, not solely the injured individual. Families approach spinal cord injuries and the onslaughts of aging differently.
The family system must be viewed for its assets and liabilities, and unique strengths need to be galvanized into action to cope with the problems of SCI. One important issue is that families often need help accommodating the changes over time as the family system ages. Families may find that their earlier solutions to problems are no longer viable and need help reframing a problem and reorganizing their family resources to generate a new solution. Again, the rehabilitation team needs to be sensitive to these ongoing, developmental aging issues within the family unit. Certainly, the issue of differential diagnosis is crucial within this population. Given the profound nature of SCI, a naïve clinician can readily project depression, despair, despondency, and resentment upon the individual with SCI. This also can happen when clinicians work with older people and so the double jeopardy of disability and age must carefully understood by any clinician working in the field. If an elderly person presents with somatic complaints or with feelings of anxiety and depression, this situation should be treated just as one would in a younger patient. Depression may not be a result of aging, but may be associated with a typical disease, psychosocial stressors, misuse of tranquilizing drugs, or use of antihypertensive. Differentiating between organic and functional etiologies especially vital in that treatment decisions are predicated upon accurate diagnoses.
It is vital that the clinician has a sound knowledge base, objective assessment, and clarity regarding his or her own potential inaccurate assumptions when contending with person who are aging/disabled. This especially applies when the clinician is called upon to make a determination regarding competency.
All fifty states and the District of Columbia have statues which define competency. There are at least 55 conditions, states, or characteristics which have been identified as defining incompetence. They range from “vicious habits,” “idleness,” and “being of unsound mind,” to “insanity” (38). Twenty-six states specifically mention “old age,” while five refer to conditions of “senility.” The Uniform Probate Code's definition of incompetent is defined as one “who is impaired by reason of mental illness, mental deficiency, physical illness or disability, advanced age, chronic use of drugs, chronic intoxication or any other cause to the extent that he lacks sufficient understanding or capacity to make or communicate responsible decisions concerning his person” (39). However, in addition to an understanding of the etiology of the incompetency, the specific parameters of potential deficit areas need to be explored.
The clinician's job is to maximize the potential independence and the autonomy of individuals with SCI and their families. People can be helped to work together and to adjust to the changes life brings by thinking of life as offering us a chance to grow rather than thinking of life's changes as losses. It is truly a question of perspective an attitude. Florida Scott-Maxwell wrote
We who are old know that age is more than a disability. It is an intense and varied experience, almost beyond our capacity at times, but sometimes to be carried high. If it is a long defeat it is also a victory, meaningful for the initiates of time, if not for those who have come less far. (40>
Clinicians have an ethical responsibility to help their clients integrate their life experience in meaningful ways and to adjust to life in the most positive ways possible. Attitudes about disabiloity and aging do impact people with SCI, and practitioners woo will need to struggle to grow and change.
REFERENCES - Section #3
SUGGESTED READING
TOP• Birren E. Schaie KW eds. Handbook of the Psychology of Aging. New York: Van No strand Reinhold, 1977, 3-12
• Birren J, Schaie K, eds. Handbook of the Psychology of Aging, 2 nd ed. New York: Academic Press, 1990, 330-346.
• Eisenberg M, Sutkin LC, Jensen MA, eds. Chronic Illness and Disability through the Life Span: Effects on Self and Family. New York: Springer Publishing Company, 1984.
• Trieschmann R. Spinal Cord Injuries: Psychological, Social and Vocational Adjustment. New York: Pergamon Press, 1980.
• Trieschmann R. Aging with a Disability. New York, Demos, 1987.
Section #4: Changing Attitude Toward Life
Gale G. Whiteneck
James, a happily married 32-year old man, has a good job as a computer programmer. He reports occasional medical problems but generally is in good health. James is treasurer of the townhouse owner's association and enjoys eating out and going to movies with his wife and attending parties and sporting events with their friends. Life is satisfying.
Most would agree that James has a good quality of life. That conclusion seems true whether or not James has a spinal cord injury (SCI). Quality of life, after all, has more to do with family, good friends, and active and productive life, and a feeling of satisfaction than it does with how physically impaired one is. On the other hand, there is no doubt that a lifetime of disability takes its toll. What is as yet unknown is how good James' quality of life will be in two or three decades.
Quality of life is often cited as the ultimate goal of rehabilitation. It is both the most important outcome from the perspective of the client and the most difficult outcome to define and measure from the prospect of the rehabilitation professional. This chapter will attempt to clarify the concept of quality of life and examine data relevant to the quality of life in individuals aging with SCI.
Quality of life is not equivalent to the absence of physiologic abnormalities and cannot be measured in terms of the severity of physical or organ system impairments. Many people with high level quadriplegia report a good quality of life (1), while many people with very incomplete paraplegia report substantial deficits in their quality of life. Using the terminology of the World Health Organization, quality of life and degree of impairment share no direct relationship. Neither is quality of life equivalent to the ability to perform activities of daily living. While the functional assessment of one's independence in activities of daily living skills is an important rehabilitation outcome Again, many individuals with minimal independence report a high quality of life while those with relatively higher levels of independence do not always consider that they have a higher quality of life.
While the concepts of impairment and disability fit well within the medical model of rehabilitation, the concept of quality of life rests more clearly within the psychosocial domain. Two distinct components of quality of life exist within this psychosocial domain. Two distinct components of quality of life exist within this psychosocial arena. First, there are the objective, observable criteria by which others evaluate the quality of our existence. For example, as others look at our lives, they evaluate where and with whom we live, if we have friends, our health, our job, and how we spend our time. From these observable factors, they draw conclusions about the quality of our lives. Second, there are the subjective perceptions we each have of the quality of our own existence. These factors have more to do with our own personal assessment of how satisfied we are with our lives than the objective criteria that others can see. The two components of quality of life, therefore, can be evaluated by the degree to which our lives meet the expectations of others and the degree to which our lives meet our own expectations.
The more objective component of quality of life might best be measured within the field of rehabilitation by the concept of handicap. As defined by the World Health Organization (2), handicap is the degree to which individuals fulfill the major social role expectations of the general society. The World Health Organization's model enumerates six dimensions or major categories of social roles:
Until recently, the measurement of handicap has either been ignored or confounded with the measurement of activities of daily living skills in disability measures. The Craig Handicap Assessment and Reporting Technique (CHART) was developed to fill this void and provide a simple objective quantification of handicap based on the World Health Organization's conceptual model (3). This tool collects behavioral data on social role fulfillment and produces scores based on normative expectations for nondisabled members of the general society. In CHART, physical independence mobility, occupation, social integration, and economic self-sufficiency are each assessed through quantifiable, objective items. These dimensions are then summed for a total handicap score.
CHART may be used to measure the objective component of quality of life – the degree to which an individual performs common social roles at a level generally expected of most nondisabled members of society. High CHART scores indicate the absence of handicap and success in achieving important social roles. These factors are certainly relevant to the more objective side of quality of life.
While CHART provides an appropriate measure of social role fulfillment from the perspective of others using the external criteria of social norms, CHART does not measure the more subjective self-perceptions of one's quality of life using one's own internal criteria. Three basic strategies have been tried to measure this component of perceived well-being:
The simplest, but least precise method employed has been the use of a single item rating scale – how would you rate your quality of life (Excellent, Good, Fair, Poor, Very Poor)?
The second strategy has used multiple item rating scales with all items focusing on the issue of perceived satisfaction with life in general. The Index of Psychological Well-Being (4) and the Life Satisfaction index (5) are examples of this approach frequently used in the psychological and gerontological literature. Both scales have been used with persons who are spinal cord injured as well as the general population. The Index of Psychological Well-Being asks people to indicate how frequently they feel certain positive and negative ways, while the Life Satisfaction Index asks how strongly people agree or disagree with positive and negative statements about life. The Life Satisfaction Index was developed to track satisfaction during the aging process.
The third strategy, developed by Flanagan (6), identified 15 quality of life categories from over 6500 critical incidence reports of individuals describing important aspects of their lives. The 15 areas included two categories of physical and material well being; four categories of relationships with others; two categories of social, community, and civic activities; four categories of personal development and fulfillment; and three categories of recreation. The Quality of Life and Individual Needs Questionnaire was then developed which asked for two separate responses to each of the 15 areas of life: (1) how important each factor was, and (2) how well needs and wants were being met. This approach provides separate assessment of both the perceived importance and the perceived fulfillment in each of 15 specific areas. The Flanagan instrument provides much more detail about one's quality of life but confines perceptions to predetermined categories rather than eliciting a global assessment.
Taken as a group, these measures provide the capability of assessing quality of life in a manner that is relevant to persons with disabilities and allow the independent measurement of both major components of quality of life – the objective component of social role fulfillment (using CHART) and the subjective component of perceived well-being (using a single question, the Index of Psychological Well-Being, the Life Satisfaction Index, and the Quality of Life and Individual Needs Questionnaire).
QUALITY OF LIFE ASSESSMENT IN THE BRITISH STUDY
All of the instruments described above were utilized as part of the reevaluation and interview process in the comprehensive British study of aging with SCI (see Chapter 3). In the study 282 persons more than 20 years post-SCI were administered the CHART, an individual item directly rating quality of life, the Index of Psychological Well-Being, the Life Satisfaction Index, and the Quality of Life and Individual Needs Questionnaire. Results from these instruments were analyzed by two age categories (35-49 and 50+ years), two categories of years post-injury (20 to 29 years post-injury and 30 or more years post-injury), and three levels of injury [persons with paraplegia of Frankel (78) grade A, B, or C indicating no functional motor sparing; persons with quadriplegia of Frankel grades A, B, or C; and all persons with SCI of Frankel grades D and E indicating very incomplete injuries with significant functional motor sparing]. Three-way analysis of variance was utilized to identify significant difference within these factors.
CHART RESULTS
Table 16.1 presents average CHART scores for the 282 individuals in the study as well as averages for sub-groups based on age, years post-injury, and level of injury. The five dimensions of handicap assessed by CHART as well as the total score are reported. Significant differences by age were identified. Total CHART scores of individuals under age 50 averaged 49 points higher than individuals 50 and over. This significant difference was mirrored in three of the five dimensions making up the total CHART score (physical independence, mobility, and occupation). While a trend in the same direction was found for social integration and economic self-sufficiency, these dimensions were not significantly different. These data indicate increasing handicap with age. Older persons with SCI report using more assistance with daily activities, having less mobility around their communities, and less time being spent in ways that society values. The fact that these differences are occurring by age 50 may indicate a relatively early withdrawal from active and productive lives among persons with SCI.
No statistically significant differences were found in any of the CHART scores when individuals injured for 20-29 years were compared with those injured for 30 or more years. This may indicate that chronological age is more closely associated with increasing handicap than is the number of years since SCI.
Table 16.1 CHART Scores by Age, Years Post-Injury (YPI), and Level of Injury |
|||||||||
|
|
By Age |
By YPI |
By Level |
|||||
Handicap Dimension |
Overall Avg. |
<50 |
50+ |
20-29 |
30+ |
Quad |
Para |
Inc |
|
Physical Independence |
90 |
93* |
88* |
89 |
94 |
74* |
96* |
98* |
|
Mobility |
81 |
88* |
76* |
82 |
80 |
71* |
82* |
92* |
|
Occupation |
73 |
83 |
65 |
75 |
67 |
64* |
75* |
79* |
|
Social Integration |
87 |
89 |
85 |
88 |
84 |
89 |
85 |
89 |
|
Economic Self-Sufficiency |
89 |
91 |
87 |
88 |
89 |
84 |
90 |
91 |
|
|
|
|
|
|
|
|
|
|
|
Total Score |
428 |
452* |
403* |
428 |
412 |
390* |
429* |
452* |
|
*Values are statistically different at the .05 level. |
|||||||||
As expected from prior research using CHART, statistically significant differences were noted by level of injury. Persons with quadriplegia were the most handicapped and individuals with very incomplete injuries were the least handicapped. Moreover, within subgroups of paraplegia and quadriplegia, the British study sample appears to average approximately 20 points lower in total CHART scores than other younger samples averaging less than 10 years post-injury. This further indicates that handicap increases during aging with SCI.
QUALITY OF LIFE QUESTION RESULTS
Interviewees in the British aging study were presented with three questions which they were asked to answer with a rating of Excellent, Good, Fair, Poor, or Very Poor:
Table 16.2 presents the frequency distribution of these five ratings.
The majority of subjects (74%) currently rate their quality of life as either good or excellent. A total of 72% indicated a similar favorable response for a period 10 years ago, but only 56% reported as favorable a response 20 years ago. This pattern indicates a general improving quality of life based on retrospective ratings.
Improvement in quality of life over time was not found in all subgroups of the sample.
Table 16.2 Quality of Life: Today, 10 Years Ago, and 20 Years Ago (in Percent) |
||||
|
Today |
10 Years Ago |
20 Years Ago |
|
Excellent |
31 |
29 |
29 |
|
Good |
43 |
43 |
27 |
|
Fair |
22 |
21 |
20 |
|
Poor |
2 |
5 |
15 |
|
Very Poor |
2 |
2 |
9 |
|
When analyzed by age, it became clear that improvement in quality of life ratings was generally isolated to the younger study group members. While those now under age 50 showed a large improvement, those 50 and over showed little change. When analyzed by years post-injury, persons more than 30 years post-injury actually reported a decline in their quality of life.
When four subgroups were formed by combining the categories of age and years post-injury, differences were even more dramatic. The largest improvement in quality of life was reported by study subjects with the least aging effect (i.e., age les than 50 and less than 30 years post-injury). The largest decline in quality of life was reported for those individuals with the greatest aging impact (i.e., 50 and over with 30 or more years post-injury). This suggests a pattern of increasing quality of life up to age 50 and 30 years post-injury, followed by slight declines in the quality of life after that point. This is similar to the findings of Creek et al. (8) in a separate study of British persons with SCI.
Psychological Well-Being Results
Table 16.3 indicates the findings for the Index of Psychological Well-Being. No statistically significant differences were found by age, years post-injury, or level of injury. However, the average results of the British study group was consistent with other groups of subjects with disabilities, showing a slightly worse index score than the average nondisabled person of similar age (4).
Table 16.3 Psychological Well-Being: |
|
Overall Average |
3.61 |
By Age |
|
35-49 |
3.77 |
50 |
3.50 |
By Years Post Injury |
|
20-29 |
3.74 |
30+ |
3.28 |
|
|
By Level of Injury |
|
Quad ABC |
3.57 |
Para ABC |
3.63 |
All Ds & Es |
3.63 |
Life Satisfaction Index Results
The results from the Life Satisfaction Index are presented in Table 16.4. Larger values indicate higher degrees of satisfaction. On this instrument, the younger age group (age 34-49) had significantly better life satisfaction than the older group (over age 50). No statistically significant differences were found by years post-injury or level of injury. Versions of the Life Satisfaction Index have been employed in various studies, including the Texas Life Status Study (9). In the investigation, satisfaction was found to be related to CHART dimensions but not to either impairment or disability.
Quality of Life and Individual Needs Questionnaire Results
Results from administration of the Quality of Life and Individual Needs Questionnaire are presented in Table 16.5. Data in the table indicate the percentage of cases reporting various dimensions as important to their quality of life and the percentage of cases reporting their needs as well met. The highest rated dimension of the study group with SCI was health and safety, with 93% indicating this was important to their quality of life. Health and safety also had the second highest percentage of respondents indicating that their needs in this area were well met. This ranking of health and safety as the most important value and the second best met need is consistent with a sample of nondisabled males 50 years old reported by Flanagan (6), who also rated health and safety the most important value and the second best met need. This is true despite the cultural differences between the British and American (6) samples, including the presence of socialized medicine in Britain.
Table 16.4 Life Satisfaction Index: |
|
Overall Average |
17.28 |
By Age* |
|
34-39 |
17.92 |
50 |
16.79 |
By Years Post Injury |
|
20-29 |
17.39 |
30+ |
16.99 |
|
|
By Level of Injury |
|
Quad ABC |
17.04 |
Para ABC |
17.32 |
All Ds & Es |
17.48 |
| *Statistically significant at the .05 level | |
Compared with the nondisabled population, the study sample of persons with SCI rated several items quite differently with regard to both relative importance and the degree to which these needs were relatively well met. In terms of importance ratings, those with SCI rated expressing themselves and reading, music, and entertainment substantially higher than did their nondisabled counterparts, but rated civic activities as substantially less important than did their nondisabled counterparts. This latter difference may reflect a cultural bias in interpreting “civic activities.” Other clear but less dramatic differences in the importance ratings included greater importance attached to helping others, learning, socializing, and active recreation by person with SCI compared with nondisabled individuals. On the other hand, the group with SCI rated material comforts, having children, and work as less important than did their nondisabled counterparts.
Regarding the degree to which various dimensions were all met, the most striking difference between individuals with SCI and those who are nondisabled was that a much lower percentage of persons with SCI indicated that having and raising children was a need that was well met. Other clear, but less dramatic, differences included lower percentages of persons with SCI indicating their needs in the areas of relationships with friends, helping others, civic activities, and work were well met.
Only a few statistically significant differences were found by the study group age. Those under age 50 rated the importance of relationships with spouses higher and reading, music, and entertainment lower than did their older counterparts. The younger group found their needs with regard to relationships with relatives better met and their needs regarding civic activities less well met than did the older group.
The main insight provided by the Quality of Life and Individual Needs Questionnaire is that the relative importance of various aspects of quality of life and the degree to which these needs are being met differs between those aging with SCI and the aging general population. Compared with the differences between persons with SCI and nondisabled individuals, differences among subgroups of individuals with SCI by age, years post-injury, and level of injury seem minor.
|
Table 16.5: Quality of Life and Individual Needs Questionnaire Results
|
|||
|
Percentage Reporting Each Dimension As: |
||
Dimensions |
Important |
Needs Well Met |
|
Material Comforts |
66 |
77 |
|
Health and Safety |
93 |
80 |
|
Relationship with Relatives |
70 |
75 |
|
Having and Raising Children |
69 |
66 |
|
Relationship with Spouse |
88 |
73 |
|
Relationship with Friends |
79 |
70 |
|
Helping Others |
81 |
58 |
|
Civic Activities |
26 |
49 |
|
Learning |
81 |
65 |
|
Understanding Yourself |
88 |
74 |
|
Work |
79 |
64 |
|
Expressing Yourself |
67 |
60 |
|
Socializing |
58 |
66 |
|
Reading, Music, Entertainment |
75 |
86 |
|
Active Recreation |
60 |
59 |
|
CORRELATIONS AMONG QUALITY OF LIFE MEASURES
The various measures used in the British study would be expected to correlate if, in fact, they measured various components of the same underlying construct – quality of life. The findings support this interpretation.
The total CHART score and all subscales except economic sufficiency were significantly correlated with the Life Satisfaction Index and the single question regarding quality of life. The physical independence dimension of CHART was significantly correlated with the Index of Psychological Well-Being. Also, the three measures of perceived well-being (the Index of Psychological well-Being, the Life Satisfaction Index, and the single quality of life question) were all significantly intercorrelated. Furthermore, several of the Flanagan quality of life dimensions were significantly correlated with the CHART dimensions and the other measures.
On the other hand, a measure of impairment – the ASIA Motor Index Score (10) was not consistently related to the quality of life measures. Only the total CHART score and the dimensions of physical independence and mobility were related. Impairment was not related to any of the perceived well-being measures. This indicates the impairment is somewhat related to the more objective component of quality of life, but not related to the more subjective component.
OTHER STUDIES OF QUALITY OF LIFE
A few other empirical investigations have focused on the issue of quality of life among aging persons with spinal cord injuries. The study which most closely matches the instruments used in the British study is an investigation conducted in Texas by the Rehabilitation Research and Training Center in Community-Oriented Services for Persons with Spinal Cord Injury (9). The Texas study found the life Satisfaction Index to be lower in the community-based sample from both urban and rural areas of southwest Texas than either the general population or previously reported spinal-cord-injured groups. Life satisfaction was related to the mobility, occupation, and social integration dimensions of CHART, but was not related to either impairment as measured by the ASIA Motor Index Score (10) or disability as measured by the Functional Independence Measure (11).
While using somewhat different instruments, research by Krause and Crew (12,13) is the only available truly longitudinal study focusing on the issues of quality of life among persons aging with SCI with data collection at multiple points in time. The work of these researchers highlight the complexity of the aging process in SCI. They found activity issues to be most strongly related with chronological age but health stability to be more related to time since injury. Both chronologic age and time since injury were correlated with some aspect of life satisfaction.
The work of Creek et al. (8) has examined the personal and social implications of SCI in England using some of the same subjects as the British study conducted by Craig Hospital in collaboration with the National Spinal Injuries Centre and Regional Spinal Injuries Centre in England. Creek et al. found that adjustment to SCI in psychological terms required considerable periods of time. Levels of expressed satisfaction increased markedly after nine years and levels of expressed dissatisfaction decreased. Creek concludes that “this cannot be explained solely in terms of the physical and psychological process of recovery; equally significant factors are the time taken to provide appropriate services, finding a suitable job, accessible accommodation and so on, and changing expectations that people have over time about living with a SCI.” Age was also found to be a significant factor. Higher levels of life dissatisfaction were associated with older ages at the time of injury. The authors recommended differing rehabilitation approaches depending upon the age of the client.
CONCLUSION
In order to adequately address the issues of quality of life in the population aging with SCI, a conceptual model is needed which differentiates objective aspects of quality of life frequently evaluated by others from the subjective perceptions of the individual utilizing his or her own personal criteria. The Craig Handicap Assessment and Reporting Technique (CHART) is recommended as an appropriate tool for assessing the more objective component of social role fulfillment while such instruments as the Index of Psychological Well-Being, the Life Satisfaction Index, and the Quality of Life and Individuals Needs questionnaire are more appropriate for assessing the subjective component of perceived well-being.
Increased handicap was found to be associated with increasing age among persons with SCI in the dimensions of physical independence, mobility, and occupation. With regard to perceived well-being, different instruments show somewhat different trends related to age and years post-injury. Clear differences, however, exist with both the relative importance of various quality of life areas and the perceived degree to which these needs are being met between persons aging with SCI and the aging general population.
The overall impression which emerges from research on quality of life among persons aging with SCI is that there is a slight increase in quality of life for several years after injury followed by slight decline over the latter period of aging. The challenge is to identify effective interventions that can help maintain a high quality of life throughout each person's lifetime. These interventions may be related to successful prevention of medical complications and functional limitations, successful modifications of equipment and environment to maintain independent and active and productive lifestyles, or education to understand and adapt to change.
ACKNOWLEDGMENTS
Portions of this chapter were prepared for an article in Paraplegia (in press) titled “Mortality, Morbidity, and Psychosocial Outcomes of Persons Spinal Cord Injured More than 20 Years Ago,” by Gale G. Whiteneck, Ph.D.; Susan W. Charlifue, M.A.; Hans L. Frankel, M.B., F.R.C.P.; Matthew H. Fraser, B.M., F.R.C.S., Kenneth A. Gerhart, M.S.; K. R. Krishnan, M.D., F.R.C.S.; Robert R. Menter, M.D.; Isaac Nuseibeh, F.R.C.S.; Deborah J. Short, M.R.C.P.; John R. Silver, M.B., B.S., F.R.C.P. Acknowledgment is extended to the coauthors for their contributions to the research, to Paraplegia for reprint permission, and to the National Institute for Disability and Rehabilitation Research for Grant H133G90010 to support this project.
REFERENCES - Section #4
Section #5: Personal Perspectives
Kenneth A. Gerhart
“All of a sudden you realize that pretty soon they're going to be deciding what in the world to do with you . . . ”
“I think it's a long time to lug around a disabled body . . . ”
“There's certainly some sadness of lost abilities, lost opportunities, maybe missed opportunities. There's also the positive side of having accumulated a lot of experiences to reflect back on, having a lot more experiences to look forward to . . . ”
THOUGHTS ON AGING AND SPINAL CORD INJURY
Do spinal cord injury survivors think about the aging process and the decades to come differently – or sooner – than their nondisabled peers? Is the aging process they experience different from that of people who are not disabled? It's difficult to say.
Sam, who has had C4 quadriplegia for over 30 years, uses a power-driven wheelchair and needs assistance for most activities of daily living. After years of living with his parents and in nursing homes, he finally got some training from an independent living program. He found an apartment and now lives alone, using attendants and other community-based support services. He attends college, enjoys working with computers, and dreams of designing software packages. Now 52 years old, he describes what most professionals and probably a lot of spinal cord injury survivors would consider significant aging-related changes. His stamina is less, his appetite fluctuates, bladder infections are worse, and he's not as limber as he once was. He has had several skin and kidney surgeries. He even says that he has grown more forgetful. “I seem to be having a lot more things go wrong, more often,” he says. Yet, surprisingly, he really doesn't believe he's aging any faster than is nondisabled peers. In fact, he says he doesn't think about aging much at all. “The only thing I think about being old is losing my hair,” he says.
Phyllis was already a wife and mother of five when an auto accident left her with quadriplegia. Twenty-five years later, she still uses a manual wheelchair. She's quite independent, but does use paid attendants in the morning and in the evening: she always has. Now, at age 65 she says, “One time I would have thought I had a good change to live into my 90s; we have longevity on both sides of my family. Probably now, chances of that are pretty slim. Anyway, I'm really healthy; I don't worry too much about that.”
Phyllis has lived with severe shoulder pain and has had surgery to repair a torn rotator cuff – a procedure she thinks was ineffective and regrets having had. On the one hand she says, “The only changes that have been detrimental for me have been the ones that had to do with my injury”; on the other hand, in what seems a blatant contradiction, she says she doesn't think her spinal cord injury has caused her body to age faster. She does not see any relationship between her orthopedic problems and her 25 years of pushing a manual wheelchair. It's almost as though she and Sam see aging as an end result rather than a process – and they're not at the end yet.
Dan apparently hasn't reached that end yet either. His bladder plagues him the way Phyllis's shoulders bother her. IN the last two or three years he has faced an increase in the frequency and severity of bladder-related problems that were severe enough to require several hospitalizations, surgery, and major changes in his bladder management program. Though his problems might logically be attributed to aging with a spinal cord injury, Dan seems unconvinced. “I don't know,” he says, “I think a lot of the complaints I hear from disabled people are the same ones I hear from nondisabled people.” So, until there is evidence to the contrary, he's going to “just kind of take it a year at a time.
So far, it seems Dan has taken not one year at a time, but 25 of them. He was injured at age 14 by a gunshot wound that left him with C6 quadriplegia. In the early years of his spinal cord injury he had multiple hospital admissions for skin repair surgery and his function was limited by calcification in his hip. The latter was so severe that it prevented him from sitting upright. When, in his late 20s he began attending college, he had to do so in a reclining power wheelchair. Now, having had surgery to remove the heterotopic ossification in his hip and having earned his degree, he has gotten married and works as a counselor at an independent living center in the Midwest–he wants nothing more than to see his 2-year old son grow up. Though he feels that this desire makes him more and more aware of his age, he's not convinced that the present state of his health is any worse than it would have been had he not been disabled.
Joe apparently feels pretty much the same way as Dan and Phyllis. He was injured 22 years ago in an automobile accident. He has low-level paraplegia and has been ambulatory most of his life. He works as a singer, songwriter, and musician. Prior to his musical career he had attended college and attempted working at “regular” jobs, but found that he always ended up with bursa problems and skin breakdowns. His music gave him the flexibility to change positions frequently and lie down if necessary. “It gave the body a real chance to keep away from problems; that seemed to work a lot better than trying to do a job.” Now, at age 40, with a brand new knee joint replacement, and other joint aches and pains, he will be relying on the wheelchair more and more. He acknowledges that he has the “bladder of a 65 or 70 year old man” and he believes that people with more problems probably age more quickly. Still, like Dan, Joe doesn't seem so sure that the problems he has are any different from ones he would have had if he hadn't sustained a spinal cord injury.
“I don't think it's like you become paraplegic or quadriplegic and instantly age 30 years.” Though it's not clear how he knows, Joe says, “I don't feel any older than I would have felt if I hadn't gotten my back broken.” He knows that he has aches and pains – but so do a lot of other people. “I remember before I got hurt, when I was 18 -- I used to worry about getting old then.”
“One thousand percent!” -- that's how strongly Art disagrees with Dan, Joe, and the others. Taking into account things other than medical problems, there is no doubt in Art's mind that his old age is very different than it would have been if it were not for his spinal cord injury 45 years ago. “I was engaged to be married,” he remembers. “Well, I've never married. I've missed that . . . They're not telling it like it is.”
In 1945, Art was 18 and only weeks away from high school graduation. He was hoping for a professional baseball career when a rollover accident left him with C4-C5 quadriplegia. After attaining what barely passed for medical stability, doctors at the Arkansas hospital told Art's parents, “Take your son home and don't bring him back.”
Two years later, Art still had not lived up to his doctors' predictions: he had failed to die. He was alive, but still totally dependent. He had skin problems and chronic bladder infections. Somehow he managed to talk his own way into a one-week rehabilitation trial at a nationally known clinic in the Midwest. He stayed a year.
Now, after over four decades with a spinal cord injury, he says, “Aging means, inside, I don't feel any older than when I was 45 . . . But on the outside, aging as a quad or a paraplegic means that you've got to be more careful . . . It means you will be weaker in body and won't be able to be up as much as you were when you were younger . . . You cannot get out and be active—in church, sports, or whatever you were active in . . . ”
Art has recently retired from 20 years in the ministry. He says that he first realized his aging concerns would be greatly worsened by his disability when his mother, his primary caregiver, became seriously ill and could no longer take care of him. “I saw that mother was not going to be able to do it and I had to have somebody come in here constantly. . . That's when I realized there was going to be quite a lot of difference. When it really, really hit me was when I lost her.”
Perhaps Art has such a different and strong opinion of aging with spinal cord injury because he is already in the midst of it all. Arguing about such things as whether aging is a process or an end result is a luxury that Art doesn't need. For Art, aging is a reality.
In several ways, Mary is very similar to Art. She, too, has been hurt almost 45 years, and sees a very definite connection between spinal cord injury and aging issues. She, too, is in the midst of an overwhelming reality.
In her early 20s and a recent college graduate about to embark on a teaching career, her auto was stuck by a drunken driver. With a C5 injury and complete quadriplegia, she was given very little hope of survival, let alone any kind of functional capability. Nonetheless, after 11 years in bed at her parents' home in rural Colorado, she was able to convince the Department of Vocational Rehabilitation to take a chance on her. She completed a physical rehabilitation program and earned a graduate degree in speech pathology. She went to work as a tutor, a speech therapist, a manager of other therapists, and later, as a patient advocate.
Early on, urinary tract infections, skin breakdown, and respiratory problems were her medical concerns. These leveled off during her working years until three years ago when a urinary tract infection sent her to the hospital. One thing led to another. Because of progressive respiratory weakness she ended up on a ventilator – despite the fact that she had what she thought was a sound living will, stating her desire to avoid artificial life support. She spent six months in the hospital.
Now, Mary has been back in her own home for about two years with around-the-clock attendant care. She is ventilator-free about 10 hours a day, but feels she must be facing a move to a nursing home sometime in the near future.
Mary clearly believes that even “normal” aging and health issues are “further complicated, or enhanced, or increased” by spinal cord injury. Of her bout with ventilator dependency, she notes, “It isn't unusual for older people to have respiratory problems of such a nature that they're using oxygen. But, I doubt that many able-bodied persons have to be on a ventilator.”
To more clearly illustrate the way she believes spinal cord injury complicates what otherwise might be normal aging, Mary uses the example of deteriorating vision. “As you grow older your vision changes and becomes more impaired. I think that's normal aging,” she says. “I think the difference for a spinal-cord-injured person is that I find that I cannot adjust the distance with what I read.” Because she is prevented from effectively moving books or newspapers farther from, or closer to, her eyes, reading has become much more difficult for her.
Like Art and Mary, Frank has no doubt that his spinal cord injury makes him approach aging differently than he would have had he not broken his neck in a skiing accident 23 years ago. He has had several recurrent shoulder injuries over the years, some with excruciating pain lasting as long as six months. Once, while traveling alone, Frank had a sudden bout with shoulder pain that virtually prevented him from transferring into his car.
In addition to these orthopedic issues, Frank, who at age 42 runs his own consulting business and travels extensively, also describes diminished energy, chronic bladder infections, progressive scoliosis and increasing spasticity. If all these problems really are caused by the spinal cord injury, Frank says, “that makes looking forward to the coming years that much more difficult . . . ” The cord injury-related aging issues are the ones that are predominant in my mind,” he adds. “And, . . .once I get past those, I still have to deal with all the other aging problems.”: When reminded that he might have had shoulder pain even if he had not had a spinal cord injury, Frank replies, “If I was able-bodied. . .I'd still be able to get around . . . Shoulder pain wouldn't be as problematic or cause as much fear for the future. "
Frank is even more concerned about his chronic bladder infections. “One thing that is truly unique to the spinal cord injury is the chronicity of the UTIs and the concern about what that bodes for me in the future . . . I'm worried about the chronic infections I've had and the chronic use of antibiotics, if that's going to present any kind of immune deficiency problems or increased severity of infections . . . I worry about the potential for cancers . . . ”
Nancy also worries about the same bladder-related issues as Frank, as well as a few other things. Now 55, Nancy was hurt over 20 years ago in a car crash. With a C6 fracture and C8 function, she's been able to be quite independent. She managed a household and raised three children herself. It wasn't until a few years ago that severe back pain caused her to switch to a power drive wheelchair. Not surprisingly, she ended up getting a van as well.
Like Frank, she also has dealt with severe shoulder pain. However, right now she is plagued most by increasingly problematic, increasingly sever, and increasingly difficult-to-treat autonomic dysreflexia. Nancy and her physicians believe that the cause of this dysreflexia problems is her aging bowel. What should be a normal aging process and a minor inconvenience instead is having a very abnormal and devastating impact. She unquestionably blames her spinal cord injury for this and many of her other aging-related problems, say the injury adds “maybe another 20 years.”
Nancy says it was the arrival of her power chair, about five years ago, that first got her thinking about the whole aging process. “I think when you get to be 50, you come to the conclusion there are fewer years ahead than there were behind, and how is spinal cord injury going to mess that up? . . . Clearly, if I was not disabled, I would feel one heck of a lot better than I do, and I would be doing a lot more . . . I think things are going to get worse; I don't think they're going to get any better.”
It was about five years ago when Jenny also began thinking about aging. At 35, Jenny is quite a bit younger than Nancy. Jenny, however, has the additional perspective of working at a spinal cord injury treatment center where she has seen countless survivors come and go–and come back again.
Fourteen years ago, at age 21, Jenny sustained T12 paraplegia. Since then she's had a baby, been divorced, attended college off and on, and has always worked at least one full-time job. Unlike many of the survivors of spinal cord injury she has seen in the course of her work, she really hasn't had any serious problems yet. She does, however, have shoulder pain, and says those joints are the parts of her body that are aging more rapidly because of her spinal cord injury. She also mentions a “new type of back pain.” Though only 35, she worries about aging with a spinal cord injury. She still sees herself as “probably better off” than most of her peers, but says “It's coming back to me that maybe you're not as strong as you used to be, and not as fast as you used to be.” Before, it was easy to actually “forget” that she was in a wheelchair; now, as she's getting older, she has to guard against such forgetting – or she's likely to end up on the floor and separated from her chair.
Mike is a lot like Jenny. He is still “youngish” but seems well aware of, and worried about, what aging holds in store for him. He also works at a spinal cord injury unit.
Mike was injured almost 20 years ago. Seventeen years old and about to enroll in one of the military academies, a tubing accident left him with quadriplegia. Since then he has lived with his parents, in a nursing home, in an apartment with a live-in attendant, and now, independently in his own home.
Like Jenny, he sees himself as “very comparable to his able-bodied peers,” and, in fact, he says, were it not for his job as a counselor to other spinal cord injury survivors – if he was “just out there in the real world” he's not sure that he'd be dealing with aging issues as much as he is. “I'm 36; that's not particularly old,” Mike says. “Yet, here I am seriously thinking about these aging issues that before I wouldn't have thought twice about.”
Though he has begun experiencing rather severe bladder difficulties in recent years, Mike worries even more about orthopedic issues, because of their impact on his independence. “The body is not designed to live its life in a wheelchair,” he says “and so I am fully expecting to have problems with shoulder and neck pain, and joint degeneration as I get older . . . I'm going to get older physically more quickly than the able-bodied population; that's just my assumption.”
Given one vote apiece, these spinal cord injury survivors seem to be quite divided on the topic of disability and aging. In fact, they seem to fall into three camps.
The first group seems to believe that aging is something that happens regardless of, and separate from, spinal cord injury. Even though some of them have significant health problems, they believe that their medical and physical status probably is no different than it would have been had they not become disabled.
Those in the second camp, on the other hand, are adamant in their belief that spinal cord injury has a profound impact on their later years. Perhaps not surprisingly, many of these individuals are themselves already in the midst of those “later years.” As a group, they believe that many of the issues they now are experiencing never would have appeared were it not for their spinal cord injuries.
Finally, the third group consists of those who still are fairly young. Most are having only one or two problems now, but are expecting more later. They do think that in the long run their spinal cord injuries will impact the aging process. Membership in this group seems to be fostered by a career in spinal cord injury health care. If these individuals can be thought of as “philosophical, but not yet card-carrying” members of the second group, the scale indeed tips in favor of those survivors who believe that spinal cord injury somehow does speed up, alter, or intensify the whole aging process.
FATIGUE: THE CUP THAT'S ONLY HALF FULL
Regardless of how they feel about aging, energy – and its likely decline – is one of the things that virtually all of these spinal cord injury survivors do think is a problem. Even those who aren't already experiencing fatigue are worrying about it. Steve, a “youngster,” and not yet complaining of other issues, says, “I'm only 31 now and already tired at the end of the day; I think even more so than I was 10 years ago.”
This “tired” person is the same one who, following a T8 injury 13 years ago that left him with complete paraplegia, went back to work the first Monday after his discharge from the rehabilitation center. He always has worked, and has gone to school off and on at the same time. He runs his own small business, maintains his own home and his own pick-up truck, and has been seen chopping his own firewood. If Steve, at 31 is “tired,” the implications of fatigue for those survivors introduced earlier may be profound.
Like Sam, for example. Because of his high level of injury, he doesn't live the active lifestyle Steve does. He never has. But he's tired too. He thinks “getting tired earlier” is his biggest problem – event bigger than the chronic bladder infections, repeated kidney surgeries, earlier bouts of skin breakdown, and unreliable attendant care he has dealt with over the past 32 years he has spent in a power drive wheelchair.
Fatigue also is very much an issue for Mary. Since her respiratory complications, she finds that her energy is so limited that she must set priorities for herself. In fact, she says that at this point, even the anticipation of a new or satisfying activity can deplete her limited energy reserves. As she describes it, “The able-bodied person starts out the day with a cup of energy; for a spinal cord injured person that cup is already reduced to probably half, so a person needs to decide how to use a half a cup of energy.” Now, she says because of aging and her other complications, that one-half cup of energy is reduced even further.
Jenny—at 35 and with “only” paraplegia to deal with—has encountered much the same thing. She used to work several jobs, but now finds that she has to cut down on the number of hours she spends working. She also needs to schedule “down time” during the middle of the day to reduce pain and conserve energy for activities that are scheduled for later in the day.
For Mike the fatigue hasn't set in yet, but he says he's expecting a certain decline in energy,” and with it “more of a need for attendant care.” He is already putting away money to pay for that attendant care and to buy the power wheelchair and van that he sees as inevitable. Frank also deals with fatigue. He figures that by his 50s or 60s he too will need a power wheelchair as well as some assistance with his personal care. Art complains of not being able to get out as much and be as active as he once was.
Clearly, fatigue is a big deal. Is it a big deal because these survivors are incredible overachievers who are just burning themselves out? Unlikely. By no one's standards is Sam an overdoer. Art and Martha stay quite active, but don't seem frenetic. The others—Steve, Frank, and Jenny—though busier than some of their peers, really aren't doing things that nondisabled people don't do. And, with 42-year-old Frank, the “granddaddy” of these three, by no stretch of the imagine can one call them “old.” Maybe the cup really isn't as full as it once was; maybe it is getting empty sooner than it should.
MAKING CHANGES
Despite fatigue and other complaints, these spinal cord injury survivors talk about “staying as active as possible.” A few have made equipment changes. Nancy, driven by back pain, now uses a power wheelchair and a van. Seemingly, the adjustment to both has been difficult. For Joe, a former full-time ambulatory who now is facing considerably more wheelchair use, the adjustment has been a great deal easier. He attributes this to the support and acceptance of his new wife. Most of the others, however, resist even these equipment changes, and none have voluntarily made changes to their activity levels.
Steve won't consider giving up his pickup truck—or his transfers to the bottom of the bath tub—even if someone were to tell him that such things, in fact, were wearing out his joints. “I don't really think there's much you can do to prevent natural-type aging.” He says. And besides, he adds “eliminating those activities doesn't sound too healthy either. If you just sit there and don't do anything . . . You probably would wither away quicker.” Despite the fact that he sounds like one of those diehard “independence at any price” people, he's not. In fact, this is the same Steve who, during his rehabilitation 13 years ago, at 19, turned to his physical therapist while in the midst of one of those bathtub transfers, and said of his disability, “You know, this is no big deal. But, what will happen to me when I get old and can't take care of myself?” Steve never has lacked insight, and never has been one who needed to deny or “overcome” his disability; he had little patience for those seemingly driven wheelchair athletes he once called “professional paras.” Actually, what Steve says pretty accurately reflects the view of many of these survivors.
Art, for example, is in his 60s and lives alone. Yet, despite his age and the limited hand and arm function caused by his quadriplegia, he says he only would give up his manual wheelchair if he were totally unable to push it anymore. Similarly, Phyllis, at age 65, with a C6 injury, chronic shoulder pain, and a failed attempt at corrective surgery, also won't give up her manual wheelchair. She says, “I feel if I had a power chair I wouldn't get any exercise at all.”
Frank also resists such changes. He fears further shoulder deterioration and increasing fatigue but puts off thinking about the power wheelchair. He wants “to be involved in many different areas of life, to push to the limits,” and feels to many adaptations will complicate his life. “I'm not as focused on wellness as much as some people are, or as much as I should be, so it's hard for me to think proactively and buy a chair now to head off a problem,” he says.
Mike like Frank, also is thinking about buying and using, at least part time, a power wheelchair to “save those shoulders.” But he hasn't made the change yet either. His reason for delaying is a little bit different. “It seems that there really isn't a definitive study out there that says, ‘yes, you're going to grow old sooner.' There are all kinds of indications—in the literature, in talking with folks – but mothering you could really pint at –just enough to make you wonder . . . ”
BUFFERS
Though it's difficult for many of these people to alter their equipment, modify their environments, or even slow down, that's not to say that their spinal cord injuries haven't cause them to think differently about the future. Most are doing quite a bit more than just “wondering.”
They worry about the inadequacy of health care, medical insurance and government support programs. They're worried about what will happen in the years to come, and they fear that in the end, they may have to make it on their own. Consequently, these survivors have begun preparing and making plans now. Nancy calls these preparatory actions “buffers.”
One of those buffers is housing. Nancy is preparing her home, making it more accessible and creating attendant quarters, so it will be able to meet her changing needs. Frank and his wife currently are building a new home. In addition to a three-car garage, designed to accommodate a future van, they also are building attendant quarters in their new home. “I don't like the idea, but I'm planning for it financially as well as practically,” says frank. Jenny also considers a home to be a crucial buffer. As a result, she is buying a townhouse that she can modify and adapt any way she wants.
Attendant care is another buffer. Dan and Phyllis both rely on spouses, and fear the financial, lifestyle, and functional implications of their spouses no longer being able to provide that care. Phyllis and her husband have responded by delaying retirement in order to continue earning the money needed to pay for attendant care.
Dan's response is a bit different. He thinks political activism is vital. “If something were to happen to her that she's not able to assist with my care,: he says of his wife, “how would I get by? I don't make enough money to pay for attendant care every day. . . May hope is that the system will adapt to my needs as I get older – health insurance, attendant care, transportation,. If all those are there for me, aging won't bother me. If they're not there, then it will bother me . . . ” So the answer for him—both personally and through his job as a counselor at an independent living center – is “becoming involved and making political changes” now.
Art should have little trouble understanding Dan's and Phyllis's concerns about attendant care. He used a family member as a caregiver for over three decades. Now he faces daily what Dan and Phyllis only fear. He and his mother had prepared many years for the time when one of them would be left alone. They saved their money and kept their household in order. Despite their preparations, however, it was his mother's illness and later her death that brought Art's own aging issues to the forefront. Everything changed. He lost his life-long companion, as well as his caregiver. Paid attendants became a part of his life. Still, the worst thing for him was, and remains, the fear that some day he will have to leave his home. “I would always tell her that if she was gone before me, I was always going to stay here as long as I could.” Now he says, “I pray that God will just let me die here at home.”
Though others aren't there yet, many have the same or similar fears. All worry about their homes and their future living situations. Those, like Mike, who don't already use attendants have begun to save for future attendant needs. In addition, virtually everyone mentions the importance of relationships – spouses, children, relatives and friends – and guards them closely. Clearly, they see these as buffers against tomorrow's physical and emotional needs.
However, there is still one more buffer – one that was mentioned so often and with such fervor that it may be more important even than those already described. That buffer is education –not the education that caregivers and rehabilitators immediately think of; not the education that has to do with learning as much as possible about their spinal cord injuries and becoming adept consumers. Instead, what comes up over and over again is the need for career-oriented education, the need for education that might increase earning power.
Earning power is what these survivors need to create a saving that will enable them eventually to buy those power wheelchairs and those vans with lifts, to pay attendants, to make up the difference between what Social Security can provide and what they think they will need to live. In short, it is earning power that will help them maintain the quality of their lives and given them the peace of mind they need.
Steve, who always saw himself involved in manual labor or construction, is tackling college in his 30s, as a means of making “a few bucks during the next 20 years or so . . . Hopefully,” he says, “I can be set up to where I can take care of myself—hire an aide, or whatever it takes.” He believes the pressure is on to produce now, while he can. “My career is going to be shortened. I think I'm going to be tired . . . I'll be 35 or 36 years old by the time I start my professional career, and I'm thinking probably twenty years and I'd be tired and ready to quit . . . A lot of things in nature decay exponentially, so I'm thinking along those lines.”
Dan also thought he'd end up in a trade, or maybe in the military. His spinal cord injury caused him to shift gears, but it wasn't until he was almost 30 that he finally got things to fall into place enough to go to college. Now, he has completed his degree, is involved in a career he enjoys, and thinks about earning a master's degree.
Sam still laments his not having been more interested in education when he was younger. At 52, he takes college courses. He still hasn't finished his degree and maybe he never will. He has never worked and probably he won't. Yet, realistic or not, he talks of some future profession as an alternative he will need to consider seriously if his government-funded home care program should change, if his eligibility should change, or if his care needs should increase. Given the instability of such programs and the fact that employment is by no means on the horizon, it's surprising that Sam isn't worrying more than he is.
Nancy, at age 55, with her children grown and off on their own, is re-starting her education process. She hopes to become an arbitrator. It's the kind of job, she says, that “I could tailor around my home and my body systems and could do in many positions . . . If you have less energy and less body ability, it's the kind of job you could still do.”
Frank and Mary, both determined years ago that education was the key for them also. Both already have completed their graduate degrees. Mary fought the system over thirty years ago to become the first client with a spinal cord injury to be funded by her state's Department of Vocational Rehabilitation. Frank finished his advanced degree while working, and still seems to wonder whether earning a doctorate might afford him even more career and financial stability.
It's interesting that so many of these survivors focus on education, career-training and self-support. Perhaps this shift was brought about by how they view the health care system and current benefit and entitlement programs, which so many spinal cord injury survivors have relied on for decades.
THE SYSTEM
These spinal cord injury survivors speak of the health care system as something from which they will need more support as they age. They believe the “system” itself, and programs like Social Security, home care allowances, and Medicaid, should be buffers against the unknowns of aging. Yet, at the same time, they are afraid to rely on such programs, for the system seems to be surrounded by as many unknowns as the aging process itself.
Mike, because of what he has seen in his role as a counselor, as well as what he has experienced personally, is more than a little concerned. “The idea of getting old and gray and having to rely on the system–Social Security and Medicare—scares me to death.” Especially, he says “when we're as reliant on the medical system as much as we are . . . I'm already putting away as much money as I can right now for things like a power wheelchair that I know I'm going to need, a van with a lift that I know I'm going to need.”
Nancy, though she feels the system has been good to her so far, and is “thankful for the programs that have been available,” still worries. Programs are “very much threatened . . . by the economy and the state of the federal government,” she says. “It's concerning for me; people who are even more dependent are under a great deal more stress about it.”
Art for one is under considerable stress. Since his mother died, he has needed substantial attendant care. The only benefit he receives is Social Security, and each monthly check covers only about a week's worth of attendant care. As a result, he pays the rest out of his own pocket. “Within three to five years all the money will be gone,” he says. “The farm will be sold, and I won't have anything. The government will just have to put me in a nursing home. That's not a very pleasant thought, but I just leave that up to the Lord.”
He's troubled by the fact that the government will not help him support himself in his own home now, but “When I don't have a dime left, they'll put me in a nursing home . . . and pay every bit of it.” This is even harder for him to understand when he figures that over all those decades of living with his mother as his caregiver, the two of them probably “saved the government a million and a half dollars – at least.”
Like Art, Mary and Phyllis are in their sixties. Both women have been battling the system for quite some time. Phyllis has her own complaints. Because of pride, personal ethics, and the fact that truly she is not a shut-in, she refuses to call herself “homebound.” This, and a few other eligibility requirements she doesn't meet, have kept her from qualifying for any of the three different elderly support programs that her small Wyoming community offers. So Phyllis and her husband, whose own arthritis is becoming increasingly a problem, have paid out of their own pockets for all the attendant care she has used since leaving the rehabilitation center 25 years ago. Their need to save money to pay for future attendant care and the difficulties of securing care while “on the road” have forced them to delay their retirement, and their plans to travel together.
Still, Phyllis's concerns shrink in comparison to the dilemmas Mary faces. Hers seems a dramatic example of the health care systems' inability to respond to the needs of the individual. It seems the system first may have let Mary down, when, for reasons that she doesn't understand, it failed to honor her living will's request that a tracheostomy not be performed.
What followed was six months of hospitalization, at a cost of over $275,000. At discharge time, with a tracheostomy in place and dependent on a mechanical ventilator, Mary was in limbo. No one, she says, knew what to do with her.
She needed 24-hour supervision because of her respiratory needs. Her private insurance coverage could not begin to pay for those expenses. As for her personal savings, Mary says, “It's very difficult to have a stocking stuffed, just from working, to prepare for the time that you no longer can work. Sometimes what you save can be a hindrance to your eligibility for other programs, and so you're caught in a Catch 22.”
For example, her Social Security was just enough to keep her from being eligible for other programs, yet not enough to really support her. Medicaid or Medicare would not pay for less expensive, non-professional providers because of the acuity of Mary's condition, yet at the same time, there was not enough money for them to pay for registered nurses. Thus, she faced a problem similar to the one Art describes. Though both agencies would pay for nursing home care, neither would commit a smaller dollar amount for home care – even though there were no appropriate local nursing homes for a person with ventilator-dependent quadriplegia anyway. Finally, through a juggling of multiple programs, and through a special foundation established by her employer, a plan was established that enabled Mary to live at home, with the round-the-clock care she needed.
Now, after about two years, this plan is beginning to fall apart. The extra funds and private donations just can't be maintained at the level needed. Mary again is looking at the possibility of a nursing home—despite the fact that she has demonstrated that she can maintain herself in her own home, safely, effectively, with a higher quality of life, and much more cheaply than in a nursing home. Even though her nursing home options are no better than they were two years ago, the government entitlement programs Mary relies on are no more flexible either. Mary says she's “not easily defeated,” but at the same time she also says she just isn't sure if it really has been worth it.
As a group, these survivors are worried about what supports they can expect from the “system” in the future. Their worries seem justified. However, in the meantime, unlike some of their peers who rely even more heavily on public support, all still are getting by. None of these survivors have reached the point where their resources are so limited they cannot even gain access to the hospital or obtain housing and other services they need. None even indicated that this was a concern; all seemed to see themselves as having or planning to have adequate resources.
Still, despite their plans, at least a few of these survivors themselves are frighteningly close to the edge and seem to be denying or ignoring that fact. A lost job, cancellation of a community-based attendant care program, an illness, changes in Medicaid or Medicare—any one of these could spell doom; any one could mean the difference between getting by and joining those who have no resources, no access to health care, and who are totally at the mercy of frequently inadequate public support programs.
It's no wonder that so many people aging with spinal cord injuries and other disabilities – especially those who know what it's like to be at the mercy of public program—are at least as afraid of the future of those programs as they are of their own increasing disabilities, fatigue, or medical problems.
QUALITY OF LIFE
In addition to Mary and Art, whose thoughts of nursing homes are more immediate than for most of the others, all of these spinal cord injury survivors discussed the possibility of such a scenario. For the majority, anti-nursing home sentiment is extremely high. For them, living in a nursing home and having a high quality of life are diametrically opposed. For a few, however, it's not the worst thing that could happen.
Sam, Dan, and Mike all have lived in nursing homes in the past. Sam is adamant in his refusal to consider a return to the nursing home; so is Dan. Dan feels quality of life is “being able to make your own decisions” – something he believes is impossible in a nursing home. “The thought of returning to one is “a nightmare . . . It would be life, but it would not be quality. I've never really thought of that ever being a possibility again . . . You have shelter and you have food, but you have no control of your life.”
Mike, on the other hand, is more philosophical. He sees his earlier nursing home days as part of his evolution into independence. He views a possible future nursing home stint as part of that same evolution. “As anybody gets older – just from a physical standpoint – you reach a pint in your life where you just can't do the same things you could do before. You need to realize you still have choices, at least in the sense of how you respond to your life's situation . . . For example, if I were to end up in a nursing home . . . I don't see the process as any different for me than anybody.” For Mike, the key to maintaining his quality of life though such changes would be to change is expectations.
Mike says that the barometer he uses to measure the quality of his life is “waking up in the morning and having those reasons to get up.” He also mentions having a job he enjoys, overall health, great family and friends, and living where he does. Though he'd like more money, he feels he has enough to meet his needs.
Others shared their own thoughts on quality of life as well. Phyllis considers quality of life to be family and friends, while Jenny says, “For me, quality of life . . . is my mental well-being . . . It's a sense of rightness I have, that all is right with the world, that I'm comfortable. It's not just material things, but that's part of it. I'm independent, I don't have to have someone take care of me; the system isn't taking care of me.”
Nancy measures quality of life in terms of family interactions, staying happy, and having some money for travel. “I want to be interested and interesting,” she says.
Although Joe sees dire financial straits as a negative, he thinks that having a nice place to live, enjoying leisure time, having “thriving and on-going” relationships, and being active and productive are important determinants of quality of life.
For Steve, like Joe, money is an issue. Quality of life is “being able to make your house payments and all your bills and still have money and time left” for other interests. He also sees working toward a goal and keeping the mind active as important contributors.
Frank has a much more aggressive view. He wants “to be fulfilled in many different areas, to be involved in many areas of life, to push the limits; to accomplish as much as you possibly can in many different areas, whether that's work, social, family, spiritual, religious.” He says that he has “an excellent quality of life compared with other cord injuries, and also compared with many, if not most” of his nondisabled acquaintances.
What could take away quality of life for these people with long term spinal cord injuries? Unremitting pain, having to be in bed, losing family and loved ones and being alone, and for some, living in a nursing home. Some hint that death or suicide might even be better than these. Even Art, a recently retired minister, says, “I think every person can reach that state, and I'm not an exception.”
Mary, who has faced the most difficult issues in this arena, thinks about quality of life a lot. Her view is uncomplicated: “If I could look at a day and think that there's something I've enjoyed, been able to do—then that one thing is a little measure of quality of life.” She says, yes, at times she has doubted whether she really has had a quality life over the past few years. Then at other times, she says, something as seemingly unimportant as looking out her window and watching a robin build a nest in the beams on her porch roof makes it all worth it . . .
FREE ADVICE
These spinal cord injury survivors have varied thoughts on quality of life and have described a range of “buffers” that they think will help them offset and prepare for what they know or believe future aging problems will be. Nonetheless, when asked to translate their thoughts in these areas into advice for others, they show surprising consensus.
First, they stress the importance of finding and keeping good care. Frank stresses the importance of finding good early rehabilitation services; Phyllis and Art both talk of the importance of good home care.
Second, they talk again about the importance of education. Steve, Sam, Nancy, and others emphasize the need for retraining and career education as a means of increasing earning power. They emphasize the need of starting such training early. Frank describes the importance of education about the spinal cord injury, and of knowing as much as possible about adaptive equipment. Dan, ever the activist, talks of the education needed to deal with the “system” “Be a better self-advocate,” he says. “I was very young when I had my injury but I've seen it happen with people who are older: basically they become manipulated by the system.”
Finally, these survivors talk of the importance of going on with the life they would have had had they not sustained spinal cord injuries. They stress the need to not change things to much. Frank, Art, and Mike all urge others to be as active as possible. Steve concurs, but adds, “Be patient” with yourself. “Live each day one at a time.”
Phyllis echoes Steve's sentiments with, “Do as much as you can of what you've always done; play it by ear.”
Mary, who hesitates to give fellow spinal cord injury survivors advice unless they specifically ask for it, would tell them to try to deal with problems “just like an able-bodied person would.”
Thoughts like these—and the various buffers against aging that these survivors of spinal cord injury describe—may be reasonable advice for those who have not yet begun to think about the decades to come. However, slowing down, taking it easy, and preserving joints, strength, and energy for later years might also be good advice. Many professionals, and certainly a few other survivors seem to be leaning toward advising the latter.
In any case, it seems that no one can ever really know exactly what to expect, especially on an individual level. Thus, no one can be totally prepared for what lies ahead. Most important, it seems that no one can ever really know when or where one of those unexpected robins' nests will turn up.
“It's an interesting process,” Mike says of aging. “I don't know how I'm going to deal with it when I grow old. It's just like having a disability: you don't know until you're there . . . ”
ACKNOWLEDGMENTS
Thanks to the survivors who shared their time, thoughts, opinions, and experiences with the author in order to make this chapter a reality.,