View Full Size Image
ARTICLE #1: PARKINSON'S DISEASE
Article Last Updated: Jul 31, 2008
TABLE OF CONTENTS
AUTHOR AND EDITOR INFORMATION
Author: Jeff Blackmer, MD, FRCP(C), Associate Professor, Medical Director, Neurospinal Service, Division of Physical Medicine and Rehabilitation, The Rehabilitation Centre; Executive Director, Office of Ethics, Canadian Medical Association
Jeff Blackmer is a member of the following medical societies: American Paraplegia Society , Canadian Association of Physical Medicine and Rehabilitation , Canadian Medical Association , and Royal College of Physicians and Surgeons of Canada
Editors: Milton J Klein, DO, MBA, Consulting Physiatrist, Sewickley Valley Hospital, Allegheny General Hospital, Harmarville Rehabilitation Center, Ohio Valley General Hospital and Aliquippa Community Hospital; Francisco Talavera, PharmD, PhD, Senior Pharmacy Editor, eMedicine; Kat Kolaski, MD, Assistant Professor, Departments of Orthopedic Surgery and Pediatrics, Wake Forest University School of Medicine; Kelly L Allen, MD , Consulting Staff, Department of Physical Medicine and Rehabilitation, Lourdes Regional Rehabilitation Center, Our Lady of Lourdes Medical Center; Denise I Campagnolo, MD, MS, Director of Multiple Sclerosis Clinical Research and Staff Physiatrist, Barrow Neurology Clinics, St. Joseph's Hospital and Medical Center; Investigator for Barrow Neurology Clinics; Director, NARCOMS Project for Consort
INTRODUCTION
James Parkinson first described Parkinson disease (PD) in 1817. PD is one of a number of chronic, progressive, neurodegenerative central nervous system ( CNS ) diseases that typically occur in adults older than 65 years. The first symptom usually is a unilateral resting tremor of the hand (pill-rolling tremor). Other common clinical features include cogwheeling rigidity, bradykinesia, and postural instability. Rigidity and bradykinesia tend to be more disabling than the tremor. The basic pathophysiology is a lack of dopamine-producing cells in the basal ganglia. This disorder can be treated both surgically and medically; physical therapy often is included in the treatment program as well, although its effectiveness remains somewhat controversial.
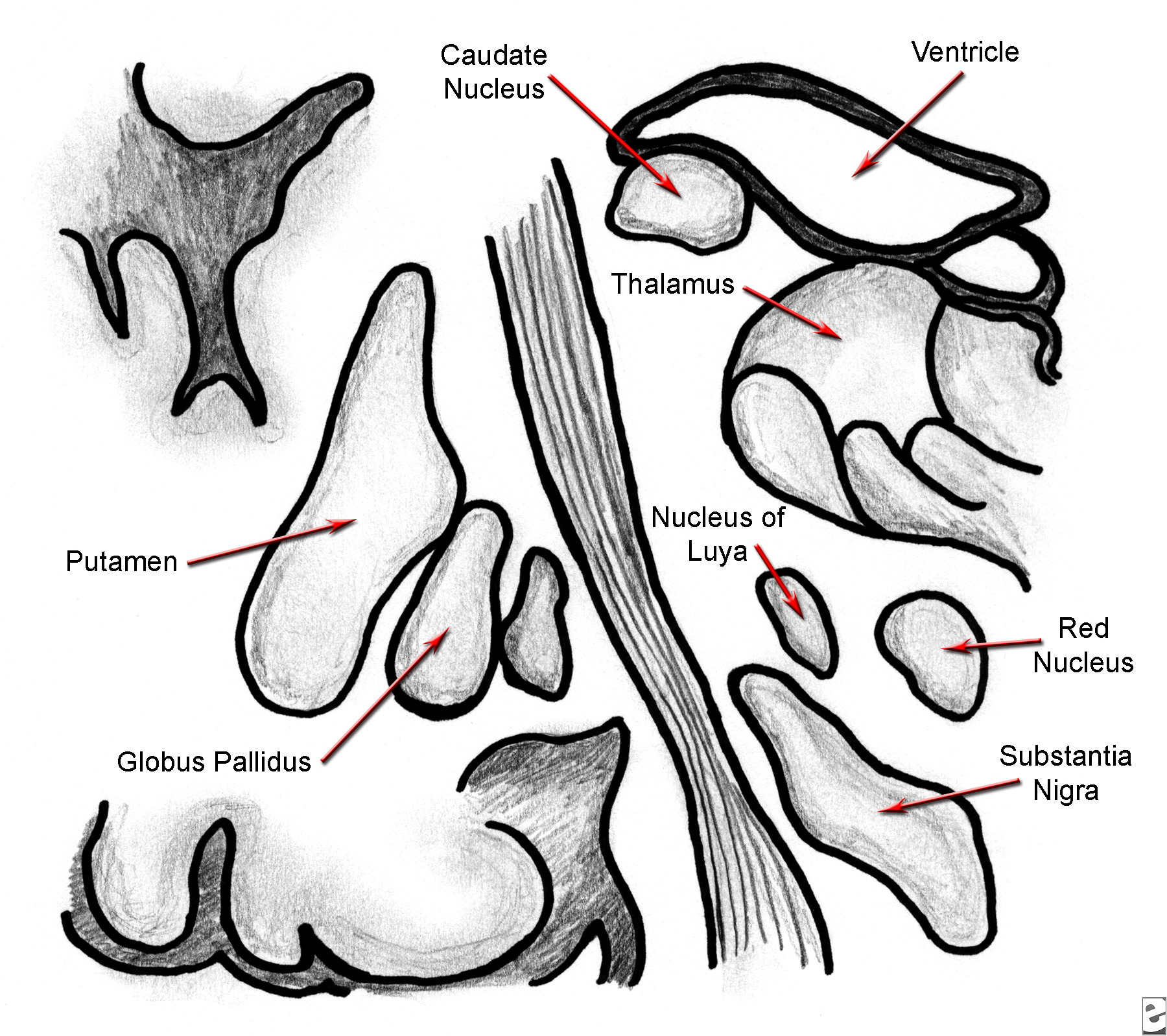
PD is a disorder of the extrapyramidal system (ie, motor structures in the basal ganglia). PD may be caused by degeneration of dopamine-producing cells in the substantia nigra, resulting in decreased levels of dopamine in the striatum. The exact effects of dopamine on movement are difficult to ascertain, in part because each of the 4 known types of postsynaptic receptors for dopamine has its own anatomic distribution and pharmacologic action. Symptoms of PD usually begin to appear when dopamine levels drop by at least 50%. Associated hyperactivity of cholinergic neurons in the caudate nuclei results in an imbalance in the normal dopamine-to-acetylcholine ratio, which contributes to the symptoms.
The exact cause of these changes remains unknown. Theories include accelerated aging, genetic susceptibility, environmental toxins (eg, cyanide, manganese, carbon disulfide, pesticides, well water, methanol, organic solvents, lead), as well as oxidative stress. The oxidative stress theory is complex and essentially involves cell death resulting from free radicals produced by oxidation of dopamine. Although the oxidative stress theory seems to receive the most support, many authors feel that the disease is probably caused by a combination of the above 4 factors.
Evidence shows that whole-body, lifetime occupational exposure to lead is an independent risk factor for the development of PD. In addition, a study conducted in Finland indicates that increasing body mass index ( BMI ) is related to an increased risk of PD development, further supporting a multifactorial and complex etiology for the condition. Please refer to Causes . Some evidence also indicates that certain environmental factors (including smoking and coffee drinking) may actually have protective associations.
United States - Frequency is similar to that found internationally.
International - Overall incidence of PD, based on several worldwide studies, is about 10-20 cases per 100,000 population per year. Prevalence estimates tend to vary, but the currently accepted figure is approximately 100-200 cases per 100,000 population.
Clinical symptoms worsen over time. Prior to the introduction of levodopa (L-dopa), PD caused severe disability or death in 25% of patients within 5 years of onset, in 65% in the next 5 years, and in 89% of those who survived for 15 years. The mortality rate from PD was 3 times that of the general population matched for age, sex, and racial origin. With the introduction of L-dopa, the mortality rate dropped approximately 50%, and longevity was extended by several years, although no evidence suggests that L-dopa actually alters the underlying pathologic process or stems the progressive nature of the disease.
Although PD is widespread, some populations seem to have a lower incidence, including the black populations of South Africa and Nigeria ; however, black persons living in Mississippi seem to be affected to the same degree as the white population. Lower incidence has also been reported in Asian populations but not in Asian Americans. Lower incidence also may not exist in the Taiwanese.
The male-to-female ratio for PD is 3:2.
The prevalence of PD increases with age. In patients younger than 40 years, the prevalence is 5 cases per 100,000 population, increasing to 300-700 cases per 100,000 population in the seventh decade and rising to more than 700 cases per 100,000 population in persons older than 70 years.
CLINICAL
Symptoms and signs of PD typically begin in one extremity or side but eventually involve the other limbs and trunk. The classic triad of PD is tremor, rigidity, and akinesia. Historical features reported by patients with PD can include the following:
Findings on physical examination in patients with PD can include the following:
The exact cause of PD remains unclear. A combination of factors probably is responsible for the condition's development. Various theories include the following:
DIFFERENTIALS
Other Problems to Be Considered
WORKUP
Diagnosis of PD is based almost entirely on results of the history and physical examination. Initial diagnostic accuracy, based on clinicopathologic studies, is about 65% (or 76% with the benefit of follow-up). In atypical cases, lab investigations may be performed to exclude other causes of parkinsonism. These investigations may include the following:
As with laboratory investigations, imaging studies and other investigations are not performed routinely for patients with clinically typical PD; however, they may assist in ruling out other causes of the patient's symptomatology.
Classic pathologic findings in PD include degeneration of the neurons containing neuromelanin, especially in the substantia nigra and the locus ceruleus. Surviving neurons often contain eosinophilic cytoplasmic inclusions called Lewy bodies. The primary biochemical defects are loss of striatal dopamine, which results from degeneration of dopamine-producing cells in the substantia nigra, as well as hyperactivity of the cholinergic neurons in the caudate nucleus.
TREATMENT
Because PD is a progressive CNS disorder with progressive disability over time, the merits of therapy often are debated. Some studies have shown benefits in certain areas (eg, gait, independence in ADL, fine motor movements) in patients receiving therapy and medication versus those receiving only medication; however, the trials generally are quite small and improvements modest. Because the studies vary in the type of therapy and medications used, the reliability of combining the results of several trials is very small.
Physical therapy often is directed at the main causes of impairment and includes measures to decrease rigidity and increase range of motion (ROM), as well as to improve postural control, endurance, mobility, and gait. Treatment of bradykinesia and rigidity often includes daily stretching and ROM exercises, as well as task-specific activities. Gait and ambulation can be improved through a program of stretching and strengthening of the lower extremities that uses exaggerated steps and arm swings, marching steps (paced to the bea t of a metronome), and mental rehearsal and imaging. The physical therapist should assess the need for ambulation aids (eg, walkers, canes) while completing gait training with the patient.
Exercises for the patient with PD should emphasize trunk extension, as well as lateral and rotational mobility, weight shifting, and balance training. Addressing how to fall safely and get up from the floor is important for patients with PD and their families. The physical therapist should instruct them in proper transfer techniques and try to improve their overall safety awareness during everyday activities. A general conditioning program also should be included in physical therapy to improve the patient's endurance. In addition, the physical therapist may instruct the patient and family members in a home exercise program.
Occupational therapy interventions include providing exercises to improve upper extremity fine motor skills and dexterity, functional training in self-care and ADL, and appropriate aids and devices, such as dressing aids (eg, reachers, sock aid), railings, grab bars, and other environmental adaptations for the home. A home visit by the therapist may be helpful.
Speech therapy may be underemployed in patients with PD, given that speech and swallowing problems are common causes of disability in this population. Speech therapy seems to improve the quality of voice in patients with hypokinetic dysarthria. Therapy itself generally emphasizes better breath and rate control, as well as improved articulation and better volume. Beneficial effects of the therapy do not seem to persist after it has been discontinued.
Dysphagia tends to occur later in the disease process and can lead to drooling, aspiration, malnutrition, and inability to ingest medications. Speech therapy interventions can include positioning the neck in flexion, teaching a double swallow technique, using smaller amounts of food, or modifying the patient's diet and incorporating thickened liquids. A modified barium swallow analysis may be helpful in guiding the therapy plan and in monitoring the patient's progress.
Because of the high level of impairment and disability seen in many patients with PD, it is not surprising that avocational pursuits for these individuals often become more difficult. This change certainly can have a detrimental impact on a patient's overall quality of life. A recreational therapist may be helpful in identifying previous recreational interests and in helping the patient to pursue them once more, with or without assistance. If such pursuits are no longer possible, new interests can be identified and explored. The therapeutic value of social and recreational pursuits should not be underestimated in patients with PD, because many of these individuals can feel isolated and lonely because of the effects of the disease.
Primary medical complications seen in patients with PD include autonomic dysfunction, cardiopulmonary impairment, dysphagia, and depression.
Interest in surgical management of PD has increased over the past few years. Three main techniques currently in use are destructive therapy (lesioning), chronic deep brain stimulation, and transplantation.
Human embryonic stem cell therapy and gene therapy
Consult with a psychiatrist for management of depression in patients who do not respond to typical treatment options, such as the use of selective serotonin reuptake inhibitors (SSRIs), or who show evidence of contemplating suicide.
MEDICATION
Medical management of PD can be quite complicated, as there are several classes of medications available, significant side effects to some of the medications, and no real consensus on which class of drug should be started at diagnosis. Different classes of medication often are combined to optimize symptom control. Medication management provides the most effective treatment of PD for the first 4-6 years. Thereafter, this disabling disease advances despite continuing medication management.
Currently, several trials are underway that are investigating potential medications for use in PD in the future. These are not yet approved for use in North America . They include symptomatic treatments targeting nondopaminergic areas, to avoid the motor complications seen with dopaminergic agents. Examples in this category include adenosine receptor antagonists and glutamate alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptor antagonists. Other agents have a neuroprotective or neurorestorative role. These include antioxidant coenzyme Q10; antiapoptotic agents, such as CEP-1347; and subthalamic glutamic acid decarboxylase, used in gene therapy.
In general, most clinicians start patients on selegiline (Eldepryl), a monoamine oxidase type B (MAO-B) inhibitor, at the time of diagnosis. This drug blocks one pathway in the breakdown of dopamine. When symptoms become more pronounced, therapy with L-dopa/carbidopa (Sinemet) or a dopamine receptor agonist (pergolide, bromocriptine) usually is instituted and is titrated as symptom control warrants, using the lowest dose required for adequate function.
Other options for medical management include anticholinergics (eg, benztropine [Cogentin]) and antivirals (eg, amantadine), which seem to have presynaptic and postsynaptic dopaminergic effects.
Some relatively new medications are available or are undergoing trials for treatment of PD. Two new dopamine agonists, ropinirole (Requip) and pramipexole (Mirapex), currently are available and may have fewer side effects than other dopamine agonists. They seem to be effective as monotherapy or in combination with other medications, such as L-dopa. A relatively new class of medications, catechol-O-methyltransferase ( COMT ) inhibitors, prevents peripheral degradation of L-dopa and allows a higher concentration to cross the blood-brain barrier. Medications in this class include tolcapone and entacapone. These medications are not widely available because of concern about elevated liver enzymes. Clinicians should see if they have been approved for use in the country where they practice.
Because of the often complicated drug regimens used by patients with PD, it is advisable to involve a neurologist with experience in management of this condition to assist with medication choice and side-effect management. Drug holidays have no basis and can be associated with significant morbidity due to a type of neuroleptic malignant syndrome.
Drug Category: Monoamine oxidase type B inhibitors
MAO-B inhibitors block one pathway in the breakdown of dopamine. This probably increases the amount of dopamine available in the brain and may prevent formation of hydrogen peroxide, offering a hypothetical neuroprotective benefit.
Drug Name |
Selegiline (Eldepryl) |
Description |
Used at time of diagnosis of PD before L-dopa therapy. May be useful as adjunct to L-dopa therapy. |
Adult Dose |
10 mg/d divided PO bid (5 mg at breakfast; 5 mg at lunch) as monotherapy or in combination with L-dopa; not to exceed 10 mg/d |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity; extrapyramidal disorders, such as excessive tremor or tardive dyskinesia; severe psychosis; profound dementia |
Interactions |
Can cause agitation and muscle rigidity and, rarely, death if taken in combination with meperidine; avoid concomitant administration of selegiline with SSRIs or TCAs; at least 5 wk should elapse between discontinuation of fluoxetine and initiation of MAOIs to prevent fatal interactions reported with MAO type A inhibitors; avoid administering MAOIs concomitantly with opioids; severe agitation, hallucinations, and death have occurred with concomitant administration of selegiline and meperidine |
Pregnancy |
C - Safety for use during pregnancy has not been established. |
Precautions |
May experience exacerbation of L-dopa – associated side effects (may need to adjust L-dopa dose accordingly); adverse reactions associated with combination of selegiline and L-dopa include hallucinations (especially visual), nausea, abdominal pain, and confusion |
Drug Name |
Rasagiline (Azilect) |
Description |
Irreversible MAO-B inhibitor that blocks dopamine degradation. Not metabolized to amphetamine derivatives. Main metabolite, aminoindan, has some activity and has been shown to improve motor and cognitive functions in experimental models. Indicated for Parkinson disease as initial monotherapy or as adjunctive therapy with levodopa. |
Adult Dose |
Monotherapy: 1 mg PO qd |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity; moderate-to-severe hepatic impairment (Child-Pugh score >6); concurrent use with meperidine, tramadol, methadone, propoxyphene; dextromethorphan, St. John's wort, mirtazapine, cyclobenzaprine, sympathomimetic amines (eg, pseudoephedrine, cocaine, ephedrine), other MAOIs, or local anesthetics containing epinephrine; pheochromocytoma |
Interactions |
P450 CYP1A2 substrate; coadministration with drugs that inhibit CYP1A2 (eg, cimetidine, clarithromycin, erythromycin) may decrease elimination and increase toxicity; coadministration with TCAs, SSRIs, serotonin-norepinephrine reuptake inhibitors (SNRIs), nonselective MAOIs, or selective MAO-B inhibitors has caused severe CNS toxicity associated with hyperpyrexia and death; consuming tyramine-rich foods (eg, cheese, red wine, beer, sausage, avocado) may cause hypertensive crisis; also see Contraindications |
Pregnancy |
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus |
Precautions |
May cause dyskinesias, hallucinations, or hypotension; if emergent surgery is necessary, benzodiazepines, mivacurium, rapacuronium, fentanyl, morphine, or codeine may be used cautiously; melanoma may develop more frequently in those taking rasagiline than in matched controls |
Drug Category: Dopaminergic agents
Because PD patients suffer from a lack of dopamine, it follows that pharmacologic therapy is directed toward dopamine replacement. Dopamine does not cross the blood-brain barrier, but L-dopa, a precursor of dopamine, does. Increasing levels of striatal dopamine through the use of L-dopa is the mainstay of medical therapy in PD. L-dopa is combined with carbidopa, which is a decarboxylase inhibitor and helps to prevent breakdown of L-dopa, thus decreasing the need for large doses of L-dopa to achieve adequate brain dopamine levels.
Drug Name |
Levodopa/carbidopa (Sinemet, Sinemet CR) |
Description |
Given together with carbidopa (a decarboxylase inhibitor) to prevent breakdown of levodopa and increase bioavailability. Decreases the need for large doses of levodopa to achieve adequate brain dopamine levels. Medications often are used when symptom control is insufficient with selegiline alone. CR formulation can help prevent the on/off phenomenon in some patients. Sinemet tablets are available in a 4:1 ratio (Sinemet 100/25) and a 10:1 ratio (Sinemet 100/10 and 250/25) of levodopa to carbidopa. Sinemet CR tablets contain a 4:1 ratio of levodopa to carbidopa (100/25 or 200/50); daily dosage of Sinemet CR must be determined by careful titration. |
Adult Dose |
Initial recommended dose is 1 tab of Sinemet CR 100/25 PO bid; in patients who require more levodopa, daily dose of 1-2 tab bid is generally well tolerated |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity; do not administer MAOIs and Sinemet concomitantly; do not administer to patients with uncompensated cardiovascular, endocrine, hematologic, hepatic, pulmonary, or renal disease or to patients with narrow-angle glaucoma; because levodopa may activate malignant melanoma, do not administer to patients with suspicious or undiagnosed skin lesions or a history of melanoma |
Interactions |
Postural hypotension can occur when given with antihypertensive drugs; dose adjustment of antihypertensive drugs may be required; phenothiazines and butyrophenones may reduce therapeutic effects of levodopa; rare reports of adverse effects resulting from concomitant use of tricyclic antidepressants and Sinemet have been made; when general anesthesia required, Sinemet should be discontinued the night before |
Pregnancy |
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus |
Precautions |
Periodic evaluations of hepatic, hematopoietic, cardiovascular, and renal function are recommended during extended therapy with Sinemet; absorption of Sinemet may be impaired in some patients on a high-protein diet |
Drug Category: Dopamine receptor agonists
Dopamine agonists directly stimulate postsynaptic dopamine receptors, bypassing the need for conversion and storage as in L-dopa therapy. These medications usually are not as effective as L-dopa in controlling symptoms of PD and typically are considered third-line medications. The 2 most commonly used medications in this class are pergolide and bromocriptine.
Drug Name |
Pergolide (Permax) |
Description |
Believed to exert therapeutic effects by direct stimulation of postsynaptic dopamine receptors in the corpus striatum. Used as an adjunct with levodopa/carbidopa for management of PD. Not recommended for treatment of newly diagnosed patients or as sole medication in PD. Pergolide was withdrawn from the US market on March 29, 2007 , because of heart valve damage resulting in cardiac valve regurgitation. It is important not to abruptly stop pergolide. Health care professionals should assess patients' need for dopamine agonist therapy and consider alternative treatment. If continued treatment with a dopamine agonist is needed, another one should be substituted for pergolide. For more information, see FDA MedWatch Product Safety Alert and Medscape Alerts: Pergolide Withdrawn From US Market . |
Adult Dose |
0.05 mg single dose PO initially for first 2 d; gradually increase by 0.1-0.15 mg/d every third day for next 12 d; then increase dosage by 0.25 mg every third d until optimal dosage achieved; administer divided doses tid |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity |
Interactions |
Dopamine antagonists, such as the neuroleptics phenothiazines, butyrophenones, thioxanthenes, or metoclopramide, may diminish effectiveness of pergolide, a dopamine agonist; because pergolide mesylate is more than 90% bound to plasma proteins, exercise caution if pergolide is coadministered with other drugs known to affect protein binding |
Pregnancy |
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus |
Precautions |
Discontinue gradually, as abrupt discontinuation may cause hallucinations and confusion; dyskinesia may occur or worsen in patients receiving levodopa with pergolide; caution in cardiac dysrhythmias; may cause or exacerbate preexisting states of confusion and hallucinations or dyskinesia |
Drug Name |
Bromocriptine (Parlodel) |
Description |
Used as adjunct therapy to levodopa in treatment of PD. Can facilitate use of lower doses of levodopa/carbidopa, thus decreasing risk of long-term complications, such as dyskinesias. |
Adult Dose |
1.25 mg PO hs initially to establish tolerance; increase to 2.5 mg/d divided bid with meals; then increase dosage prn, adding an additional 2.5 mg/d, once q2-4wk taken in 2-3 divided doses with meals |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity; coronary artery disease; severe cardiovascular disorders |
Interactions |
Adverse effects may increase if coadministered with ergot alkaloids, erythromycin, or sympathomimetic agents; coadministration with dopamine antagonists (eg, metoclopramide), phenothiazines, butyrophenones (eg, haloperidol), pimozide, amitriptyline, imipramine, methyldopa, or reserpine may decrease efficacy |
Pregnancy |
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals |
Precautions |
May cause postural hypotension; periodic monitoring of blood pressure advisable; dizziness; caution patients about driving until response determined; few cases of GI bleeding and ulceration reported; discontinue medication if this occurs; safety not established in patients with severe hepatic or renal disease |
Drug Name |
Apomorphine (Apokyn) |
Description |
Elicits dopamine agonist effect. Indicated to treat acute immobility episodes (hypomobility or "off-periods") in PD. These episodes consist of inability to rise from a chair, speak, or walk and may occur toward the end of the dose interval or may be spontaneous and unpredictable in onset. Approximately 10% of individuals with stage IV PD who do not respond to standard medications for acute immobility may respond to apomorphine. |
Adult Dose |
Dosage is individualized |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity to apomorphine or metabisulfite |
Interactions |
Coadministration with 5HT3 antagonists used for emesis or irritable bowel syndrome (eg, ondansetron, dolasetron, granisetron, palonosetron, alosetron) may cause hypotension and loss of consciousness; coadministration with drugs that increase QTC interval (eg, thioridazine, quinidine, sotalol, erythromycin, dofetilide) may increase arrhythmia potential; metabolized by COMT , coadministration with COMT inhibitors (eg, entacapone, tolcapone) may decrease elimination |
Pregnancy |
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus |
Precautions |
Causes severe nausea and vomiting and must be administered with an antiemetic drug (but not with antiemetic agents that are 5HT3 antagonists); may cause orthostatic hypotension, faintness, hallucinations, fluid retention, chest pain, increased sweating, flushing, pallor, dyskinesia, rhinorrhea, and extreme drowsiness (may fall asleep during waking hours without warning) |
Drug Name |
Rotigotine (Neupro) |
Description |
April 2008: A recall was issued for Neupro patch in the United States because of crystal formation in the patch that resulted in decreased dopamine absorption transdermally. As of August 1, 2008 , the patch was still unavailable, although the manufacturer is working to correct the defect and return the product to the market. For more information see Medscape News . |
Adult Dose |
2 mg/24 h (10 cm 2 ) transdermal qd initially; may increase qwk by 2 mg/24 h, not to exceed 6 mg/24 h |
Pediatric Dose |
Indication not applicable to children |
Contraindications |
Documented hypersensitivity |
Interactions |
Dopamine antagonists (eg, antipsychotics, metoclopramide) may decrease effect |
Pregnancy |
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus |
Precautions |
Common adverse effects include dermal reactions at patch site, dizziness, nausea, vomiting, drowsiness, and insomnia; less common adverse effects that may be hazardous to patient include sudden sleep onset, hallucinations, and postural hypotension; weight gain secondary to fluid retention has been observed; rapid dose reduction or abrupt withdrawal may cause hyperpyrexia and confusion; apply to clean, dry, and intact skin on abdomen, thigh, hip, flank, shoulder, or upper arm |
Drug Category: Anticholinergics
The most commonly used treatment for PD until the introduction of L-dopa; it probably works by blocking cholinergic receptors in the striatum and restoring the dopamine-acetylcholine balance; benztropine (Cogentin) is the most common anticholinergic agent in the treatment of PD.
Drug Name |
Benztropine (Cogentin) |
Description |
May be effective at any stage of disease process; helpful in patients resistant to other agents; reduces tremor and rigidity. |
Adult Dose |
1-2 mg/d with range of 0.5-6 mg PO or parenterally; 0.5-1 mg hs; individualized treatment required; smaller doses likely in older or thinner patients |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity; glaucoma |
Interactions |
Decreases effects of levodopa; increases effects of narcotic analgesics, phenothiazines, quinidine, tricyclic antidepressants, and anticholinergics |
Pregnancy |
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus |
Precautions |
May cause weakness or inability to move particular muscle groups in larger doses; mental confusion and visual hallucinations may occur; tardive dyskinesia reported in long-term benztropine use; caution in hot weather because of anhidrosis; advise patient to report GI complaints, fever, or heat intolerance if concomitantly administered with phenothiazines, haloperidol, or other drugs with anticholinergic or antidopaminergic activity; paralytic ileus reported in patients taking benztropine in combination with phenothiazines and/or tricyclic antidepressants |
Drug Category: Antivirals
Amantadine (Symmetrel) is the only antiviral used in the treatment of PD. The mechanism of action is unknown; it may trigger the release of brain dopamine from nerve endings.
Drug Name |
Amantadine (Symmetrel) |
Description |
Used alone and in combination with anticholinergic antiparkinsonian medications and with levodopa/carbidopa; maximal therapeutic benefit usually occurs within 1 wk, and initial benefits may decrease with continued dosing. May be useful as adjunct in patients who do not tolerate optimal doses of levodopa alone or in combined therapy with carbidopa. Amantadine may result in better control of PD in these patients and may decrease fluctuations in performance. |
Adult Dose |
100 mg/d PO initially; after a few wk may be increased to 100 mg bid; increase to 300 mg/d divided dose may help some patients |
Pediatric Dose |
Not established |
Contraindications |
Documented hypersensitivity |
Interactions |
Drugs with anticholinergic or CNS stimulant activity increase amantadine toxicity; the concurrent administration of hydrochlorothiazide plus triamterene with amantadine may increase plasma concentrations of amantadine |
Pregnancy |
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus |
Precautions |
Parkinsonian crisis may result from abrupt discontinuation; neuroleptic malignant syndrome associated with dose reduction or withdrawal of amantadine; reduce dose in patients with renal impairment and in patients aged 65 y or older; exercise care in patients with congestive heart failure, liver disease, orthostatic hypotension, or psychosis |
FOLLOW-UP
Underlying medical illness (eg, sepsis, pneumonia, fecal impaction, urinary tract infection) should be suspected in a PD patient with a rapid deterioration or new PD symptoms. </li>
Prognosis is discussed in Mortality/Morbidity .
REFERENCES
Article Last Updated: Jul 31, 2008